

Percutaneous Tibial Nerve Stimulation for Neurogenic Bladder Due to Severe Lumbosacral Disc Herniation
- PMID: 40217712
- PMCID: PMC11989787
- DOI: 10.3390/jcm14072262
Percutaneous Tibial Nerve Stimulation for Neurogenic Bladder Due to Severe Lumbosacral Disc Herniation
Abstract
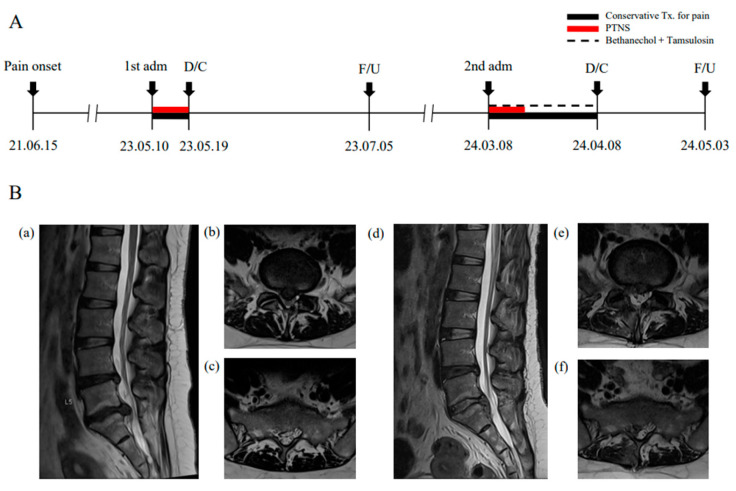
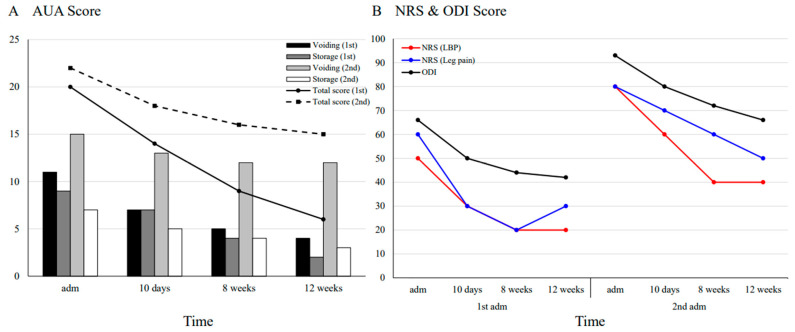
Background: Neurogenic bladder (NB), resulting from neurological disorders, significantly affects quality of life and increases healthcare costs. Although percutaneous tibial nerve stimulation (PTNS) is an established therapy for central nervous system-related lower urinary tract dysfunction (LUTD), its efficacy in treating intervertebral discogenic LUTD remains unexplored. This study presents the first documented case of PTNS applied to NB secondary to severe lumbosacral herniated intervertebral disc (HIVD). Methods: A 39-year-old female, hospitalized twice for worsening HIVD, presented with LUTD, including urgency, weak stream, and nocturia. Magnetic resonance imaging confirmed progressive L5-S1 disc extrusion with sacral nerve compression. PTNS, delivered via electronic stimulation through acupuncture needles at SP6 and KI3, was administered daily for 10 days during hospitalization. Symptom scores relating to LUTD, pain, and physical disability were evaluated. Result: The American Urological Association symptom score showed significant improvement (from 20 to 6 and 22 to 15 at 12 weeks after the first and second hospitalizations, respectively). Recovery of voiding function was slower during the second hospitalization, possibly due to increased sacral nerve compression and chronic pathologic condition. Pain and functional disability, assessed using the NRS and ODI, improved by approximately 50% (from 55 to 25 and 80 to 45 during the first and second hospitalizations, respectively) and two-thirds (from 66 to 42 and 93 to 66, respectively). Conclusions: This case suggests that PTNS may be a viable conservative therapy for HIVD-associated LUTD. Further research is required to elucidate its mechanistic effects and clinical efficacy in peripheral nerve-related bladder dysfunction.
Keywords: PTNS; case report; herniated disc; neurogenic bladder.
Conflict of interest statement
The authors declare that this research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of posterior tibial nerve stimulation (PTNS) on lower urinary tract dysfunction: An umbrella review.Neurourol Urodyn. 2024 Feb;43(2):494-515. doi: 10.1002/nau.25343. Epub 2023 Dec 28. Neurourol Urodyn. 2024. PMID: 38153131
-
Efficacy and Safety of Sacral and Percutaneous Tibial Neuromodulation in Non-neurogenic Lower Urinary Tract Dysfunction and Chronic Pelvic Pain: A Systematic Review of the Literature.Eur Urol. 2018 Mar;73(3):406-418. doi: 10.1016/j.eururo.2017.11.002. Epub 2018 Jan 12. Eur Urol. 2018. PMID: 29336927 Review.
-
Percutaneous Tibial Nerve Stimulation Improves Lower Urinary Tract Dysfunction and Infection Rate in a Kidney Transplant Recipient With Augmentation Cystoplasty: A Case Report and Literature Review.Transplant Proc. 2022 Dec;54(10):2727-2729. doi: 10.1016/j.transproceed.2022.08.049. Epub 2022 Oct 30. Transplant Proc. 2022. PMID: 36319495 Review.
-
Efficacy of percutaneous and transcutaneous tibial nerve stimulation in women with idiopathic overactive bladder: A prospective randomised controlled trial.Ann Phys Rehabil Med. 2022 Jan;65(1):101486. doi: 10.1016/j.rehab.2021.101486. Epub 2021 Nov 11. Ann Phys Rehabil Med. 2022. PMID: 33429090 Clinical Trial.
-
Predictors of successful percutaneous tibial nerve stimulation (PTNS) in the treatment of overactive bladder syndrome.Int Urogynecol J. 2019 Oct;30(10):1735-1745. doi: 10.1007/s00192-018-3834-9. Epub 2018 Nov 29. Int Urogynecol J. 2019. PMID: 30498931
References
-
- Przydacz M., Denys P., Corcos J. What do we know about neurogenic bladder prevalence and management in developing countries and emerging regions of the world? Ann. Phys. Rehabil. Med. 2017;60:341–346. - PubMed
-
- Ogawa T., Yoshimura N. Essentials of the Adult Neurogenic Bladder. CRC Press; Boca Raton, FL, USA: 2020. Pathologies of the Basal Ganglia, such as Parkinson’s and Huntington’s Diseases; pp. 71–77.
-
- Manack A., Motsko S.P., Haag-Molkenteller C., Dmochowski R.R., Goehring E.L., Jr., Nguyen-Khoa B.A., Jones J.K. Epidemiology and healthcare utilization of neurogenic bladder patients in a US claims database. Neurourol. Urodyn. 2011;30:395–401. - PubMed
-
- De Sèze M., Ruffion A., Denys P., Joseph P.-A., Perrouin-Verbe B., GENULF The neurogenic bladder in multiple sclerosis: Review of the literature and proposal of management guidelines. Mult. Scler. J. 2007;13:915–928. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
