

Does Preliminary Chest Shape Assessment Improve the Prognostic Risk Stratification of Individuals with Mitral Annular Disjunction? A Case Report and Narrative Review
- PMID: 40217727
- PMCID: PMC11989957
- DOI: 10.3390/jcm14072277
Does Preliminary Chest Shape Assessment Improve the Prognostic Risk Stratification of Individuals with Mitral Annular Disjunction? A Case Report and Narrative Review
Abstract
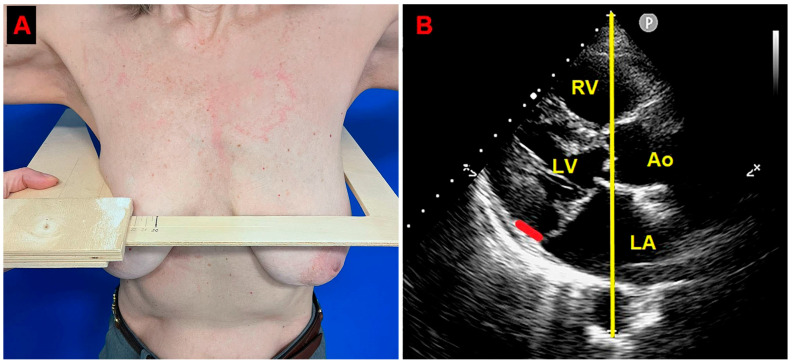
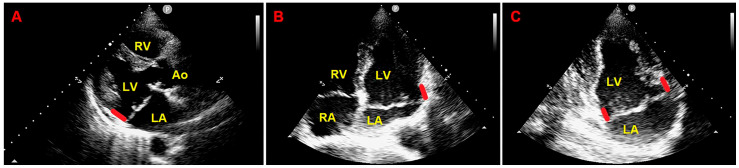
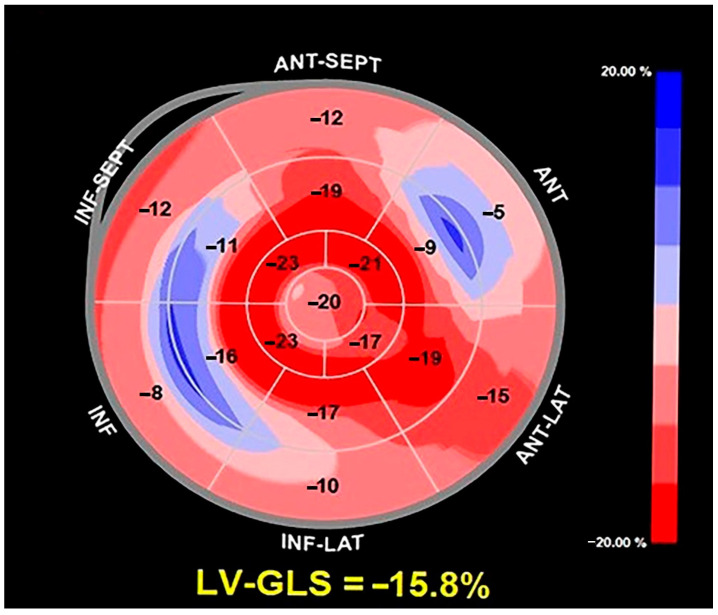
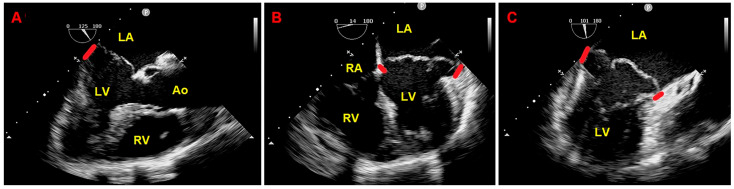
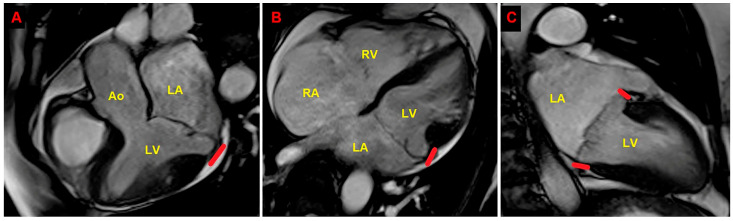
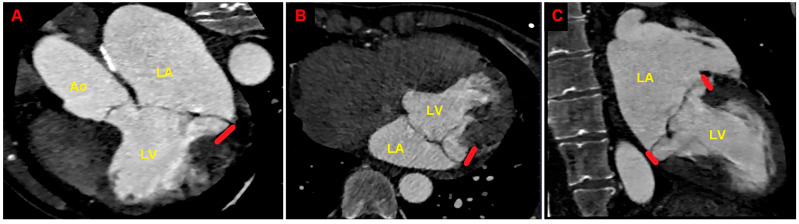
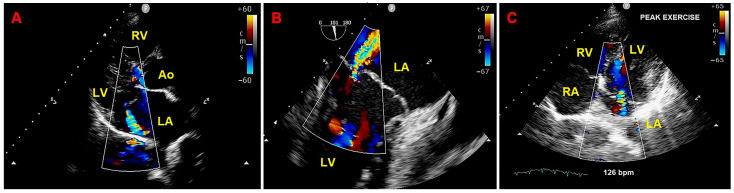
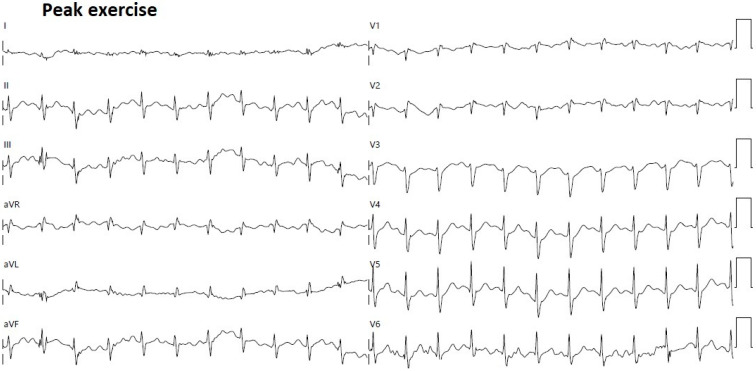
Background: Mitral annular disjunction (MAD), a mitral annular abnormality involving the whole mitral valve annulus circumference, commonly detected in individuals with mitral valve prolapse (MVP), has been recently recognized as a potential risk factor for malignant ventricular arrhythmias (VAs) and sudden cardiac death. Recent evidence indicates that a multimodality imaging assessment comprehensive of echocardiography, cardiac magnetic resonance (CMR), and cardiac computed tomography angiography (CCTA) may improve MAD detection. To date, no previous author has considered the potential influence of chest wall conformation on MAD presence. Considering the strong association between MVP and anterior chest wall deformities and the increased prevalence of MAD among MVP individuals, we have hypothesized that MAD presence might be more frequently detected among MVP individuals with a narrow anteroposterior (A-P) thoracic diameter and/or concave-shaped chest wall conformation, as noninvasively assessed by the modified Haller index (MHI). Methods: Herein, we present a case of MVP female with relevant MAD distance and moderate mitral regurgitation (MR) who underwent a diagnostic study comprehensive of transthoracic echocardiography, transesophageal echocardiography, CMR, CCTA, and exercise stress echocardiography. Results: The patient was found with a concave-shaped chest wall conformation (MHI > 2.5) and narrow A-P thoracic diameter (<13.5 cm), with a moderate and non-hemodynamically significant MR, without areas of LGE on CMR and with low arrhythmic profile. Conclusions: A preliminary chest shape assessment by the MHI might improve the prognostic risk stratification of MVP patients with MAD, potentially identifying a benign phenotype of MVP individuals, i.e., those with a narrow A-P thoracic diameter.
Keywords: arrhythmic burden; mitral annular disjunction; mitral valve prolapse; modified Haller index; multimodality imaging assessment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
The influence of chest wall conformation on myocardial strain parameters in a cohort of mitral valve prolapse patients with and without mitral annular disjunction.Int J Cardiovasc Imaging. 2023 Jan;39(1):61-76. doi: 10.1007/s10554-022-02705-w. Epub 2022 Aug 6. Int J Cardiovasc Imaging. 2023. PMID: 36598688
-
The Prevalence, Pathophysiological Role and Determinants of Mitral Annular Disjunction Among Patients with Mitral Valve Prolapse: A Systematic Review.J Clin Med. 2025 Feb 20;14(5):1423. doi: 10.3390/jcm14051423. J Clin Med. 2025. PMID: 40094868 Free PMC article. Review.
-
Role of cardiac magnetic resonance in stratifying arrhythmogenic risk in mitral valve prolapse patients: a systematic review and meta-analysis.Eur Radiol. 2024 Nov;34(11):7321-7333. doi: 10.1007/s00330-024-10815-3. Epub 2024 Jun 6. Eur Radiol. 2024. PMID: 38844620 Free PMC article.
-
The Mitral Annulus Disjunction Arrhythmic Syndrome.J Am Coll Cardiol. 2018 Oct 2;72(14):1600-1609. doi: 10.1016/j.jacc.2018.07.070. J Am Coll Cardiol. 2018. PMID: 30261961
-
Prevalence of Diastolic and Systolic Mitral Annular Disjunction in Patients With Mitral Valve Prolapse.J Am Soc Echocardiogr. 2025 Jan;38(1):1-11. doi: 10.1016/j.echo.2024.10.004. Epub 2024 Oct 21. J Am Soc Echocardiogr. 2025. PMID: 39442734
References
-
- Van der Bijl P., Stassen J., Haugaa K.H., Essayagh B., Basso C., Thiene G., Faletra F.F., Edvardsen T., Enriquez-Sarano M., Nihoyannopoulos P., et al. Mitral Annular Disjunction in the Context of Mitral Valve Prolapse: Identifying the At-Risk Patient. JACC Cardiovasc. Imaging. 2024;17:1229–1245. doi: 10.1016/j.jcmg.2024.03.006. - DOI - PubMed
-
- Figliozzi S., Stankowski K., Tondi L., Catapano F., Gitto M., Lisi C., Bombace S., Olivieri M., Cannata F., Fazzari F., et al. Mitral Annulus Disjunction in consecutive patients undergoing Cardiac Magnetic Resonance: Where is the boundary between normality and disease? J. Cardiovasc. Magn. Reson. 2024;26:101056. doi: 10.1016/j.jocmr.2024.101056. - DOI - PMC - PubMed
-
- Sonaglioni A., Nicolosi G.L., Muti-Schünemann G.E.U., Lombardo M., Muti P. The Prevalence, Pathophysiological Role and Determinants of Mitral Annular Disjunction Among Patients with Mitral Valve Prolapse: A Systematic Review. J. Clin. Med. 2025;14:1423. doi: 10.3390/jcm14051423. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
