

Identification of Perioperative Risk Factors for Early Sacral Nerve Stimulator Explantation: A Single-Center Retrospective Cohort Study
- PMID: 40217812
- PMCID: PMC11989564
- DOI: 10.3390/jcm14072363
Identification of Perioperative Risk Factors for Early Sacral Nerve Stimulator Explantation: A Single-Center Retrospective Cohort Study
Abstract
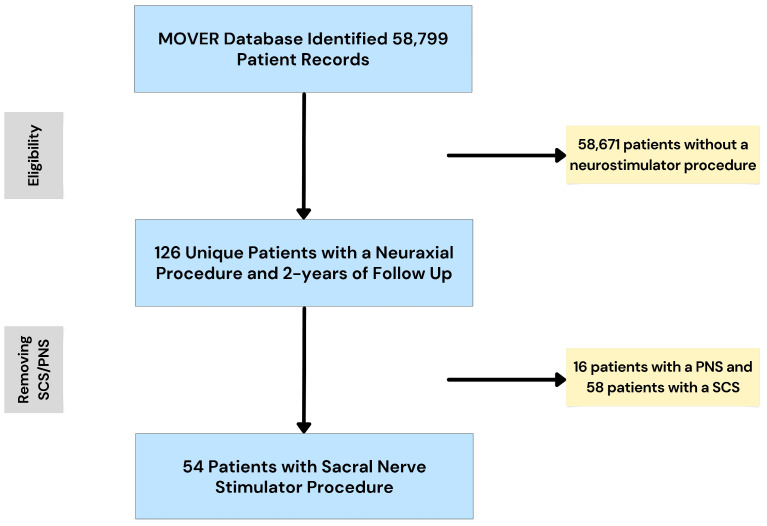
Background: Sacral nerve stimulators (SNSs) can be an effective treatment for urinary incontinence. However, with a failure rate of up to 50%, an explantation rate of up to 16%, and a cost of ~USD 10,000 per implant, identification of patients at high risk for explantation is necessary to improve patient satisfaction and reduce the economic burden on the healthcare system. The objective of this retrospective cohort study was to determine predictors of SNS explantation within the first two years of device placement. Methods: The MOVER database was queried for patients with a SNS and at least two years of follow-up (n = 54). Multivariate logistic regression was performed to assess risk factors for explantation. Factor optimization was used to eliminate factors with limited predictive value. Results: The model displayed excellent performance with an AUC of 0.93 (95% CI: 0.78-1.00) and an f1-score of 0.81. Female sex (OR: 3.75; CI: 3.71-3.79), malignancy (OR: 3.14; CI: 3.10-3.18), ASA score (OR: 2.53; CI: 2.50-2.57), peripheral neuropathy (OR: 2.04: CI: 2.01-2.07), alcohol use (OR: 1.98; CI: 1.96-2.01), and length of stay (OR: 1.47; CI: 1.45-1.49) displayed statistically significant increased risk of explantation. Atrial fibrillation (OR: 0.36; CI: 0.35-0.36) and chronic kidney disease (OR: 0.54; CI: 0.53-0.54) were included in the model but conferred decreased risk of explantation. Conclusions: Patient ASA score and a medical history of malignancy, peripheral neuropathy, and alcohol use are possible novel risk factors for SNS explantation.
Keywords: chronic pain management; explantation surgery; sacral nerve stimulator; surgical indication; urinary incontinence.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Sacral nerve stimulation for urinary urge incontinence, urgency-frequency, urinary retention, and fecal incontinence: an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(3):1-64. Epub 2005 Mar 1. Ont Health Technol Assess Ser. 2005. PMID: 23074472 Free PMC article.
-
Evaluation of Sacral Nerve Stimulation Device Revision and Explantation in a Single Center, Multidisciplinary Study.Neuromodulation. 2020 Dec;23(8):1201-1206. doi: 10.1111/ner.13050. Epub 2019 Nov 7. Neuromodulation. 2020. PMID: 31697433
-
Comparison of long-term outcome of sacral nerve stimulation for constipation and faecal incontinence with focus on explantation rate, additional visits, and patient satisfaction.Tech Coloproctol. 2020 Nov;24(11):1189-1195. doi: 10.1007/s10151-020-02328-0. Epub 2020 Aug 27. Tech Coloproctol. 2020. PMID: 32856184
-
Treatment of the infected sacral nerve stimulator: A scoping review.Neurourol Urodyn. 2024 Mar;43(3):579-594. doi: 10.1002/nau.25411. Epub 2024 Feb 6. Neurourol Urodyn. 2024. PMID: 38318878
-
Pediatric vagal nerve stimulator explantation: A comprehensive literature review and tertiary care experience.Int J Pediatr Otorhinolaryngol. 2023 Jul;170:111603. doi: 10.1016/j.ijporl.2023.111603. Epub 2023 May 29. Int J Pediatr Otorhinolaryngol. 2023. PMID: 37267661 Review.
Cited by
-
Perioperative Predictors of Early Spinal Cord Stimulator Removal: A Retrospective Cohort Study.Neurol Int. 2025 Jun 27;17(7):100. doi: 10.3390/neurolint17070100. Neurol Int. 2025. PMID: 40710903 Free PMC article.
-
Optimizing Multivariable Logistic Regression for Identifying Perioperative Risk Factors for Deep Brain Stimulator Explantation: A Pilot Study.Clin Pract. 2025 Jul 17;15(7):132. doi: 10.3390/clinpract15070132. Clin Pract. 2025. PMID: 40710042 Free PMC article.
References
-
- Gajewski J.B., Schurch B., Hamid R., Averbeck M., Sakakibara R., Agro E.F., Dickinson T., Payne C.K., Drake M.J., Haylen B.T. An International Continence Society (ICS) report on the terminology for adult neurogenic lower urinary tract dysfunction (ANLUTD) Neurourol. Urodyn. 2018;37:1152–1161. doi: 10.1002/nau.23397. - DOI - PubMed
LinkOut - more resources
Full Text Sources
