

The Enhanced Recovery After Surgery Pathway Is Safe, Feasible and Cost-Effective in Delayed Graft Function After Kidney Transplant
- PMID: 40217837
- PMCID: PMC11990043
- DOI: 10.3390/jcm14072387
The Enhanced Recovery After Surgery Pathway Is Safe, Feasible and Cost-Effective in Delayed Graft Function After Kidney Transplant
Abstract
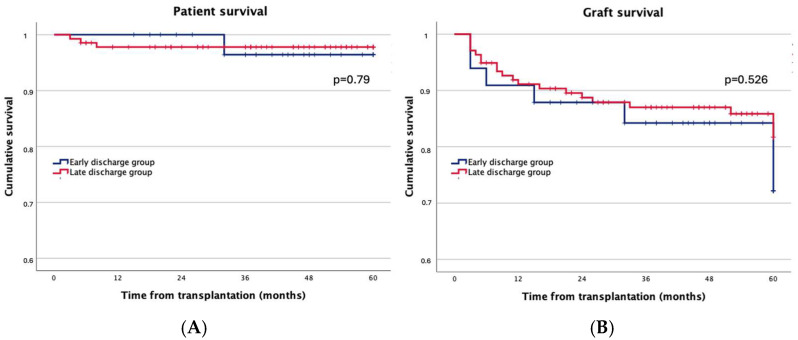
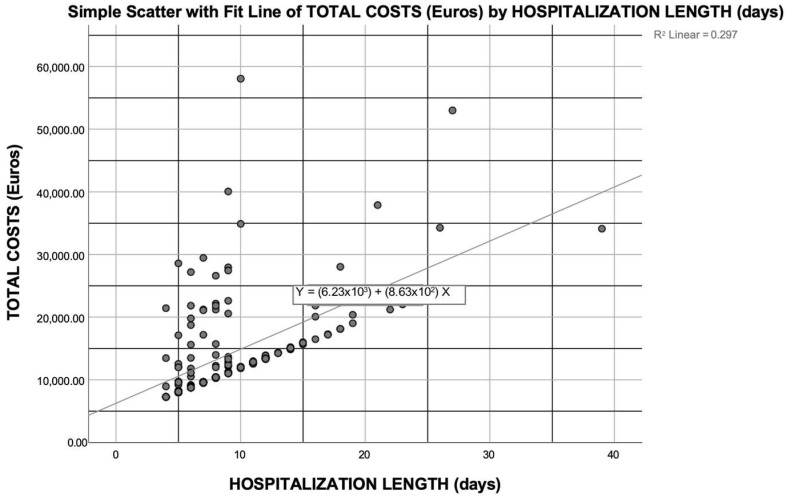
Background/Objectives: Enhanced recovery after surgery (ERAS) pathways are still underutilized in kidney transplantation (KT), and their feasibility after delayed graft function (DGF) is unknown. We aimed to evaluate safety and cost savings after ERAS implementation in KT recipients with DGF. Methods: A retrospective analysis of KT recipients enrolled in the ERAS program with DGF (≥1 dialytic treatment during the first postoperative week or creatinine≥ 2.5 mg/dL on postoperative day 10) between 2010 and 2019 was performed. Recipient, donor, and transplant data, outcomes, and 1-year post-KT costs were collected, comparing recipients within the ERAS target (≤5 days, "early discharge group") to those discharged later (>5 days, "late discharge group"). Results: Out of 170 KT recipients with DGF, 33 (19.4%) were in the "early discharge group" and 137 (80.5%) in the "late discharge group". Recipient, donor, and transplant characteristics were similar in the two groups. The length of hospital stay (LOS) of the "early discharge group" was significantly shorter, with fewer in-hospital dialysis sessions (p < 0.001) compared to the "late discharge group". One year post-KT, no significant differences were observed in postoperative complications, readmissions, or number of outpatient visits. Five-year graft and patient survival along with five-year graft function were similar between the two cohorts. First-year costs were significantly higher in the "late discharge group" (p < 0.001), with a median excess cost (Δ) of EUR 4515.76/patient. Factors influencing first-year costs post-KT were LOS for KT, recipient age, and use of expanded-criteria grafts. Conclusions: The ERAS approach is safe in KT recipients with DGF and allows for economic savings, while its implementation does not cause worse clinical outcomes in recipients.
Keywords: cost-effectiveness; delayed graft function; enhanced recovery after surgery protocols; healthcare costs; kidney transplantation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Ljungqvist O., Scott M., Fearon K.C. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017;152:292–298. - PubMed
-
- Gustafsson U.O., Scott M.J., Hubner M., Nygren J., Demartines N., Francis N., Rockall T.A., Young-Fadok T.M., Hill A.G., Soop M., et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations. World J. Surg. 2019;43:659–695. - PubMed
-
- Greco M., Capretti G., Beretta L., Gemma M., Pecorelli N., Braga M. Enhanced Recovery Program in Colorectal Surgery: A Meta-analysis of Randomized Controlled Trials. World J. Surg. 2014;38:1531–1541. - PubMed
-
- ERAS Society (2022) [(accessed on 31 December 2024)]. Available online: https://erassociety.org/guidelines/
LinkOut - more resources
Full Text Sources
