

Clinical Outcome of Endoscopic and Endoscopic-Assisted Microscopic Removal of Glomus Tympanicum: A Multicenter Retrospective Study
- PMID: 40217838
- PMCID: PMC11989738
- DOI: 10.3390/jcm14072388
Clinical Outcome of Endoscopic and Endoscopic-Assisted Microscopic Removal of Glomus Tympanicum: A Multicenter Retrospective Study
Abstract
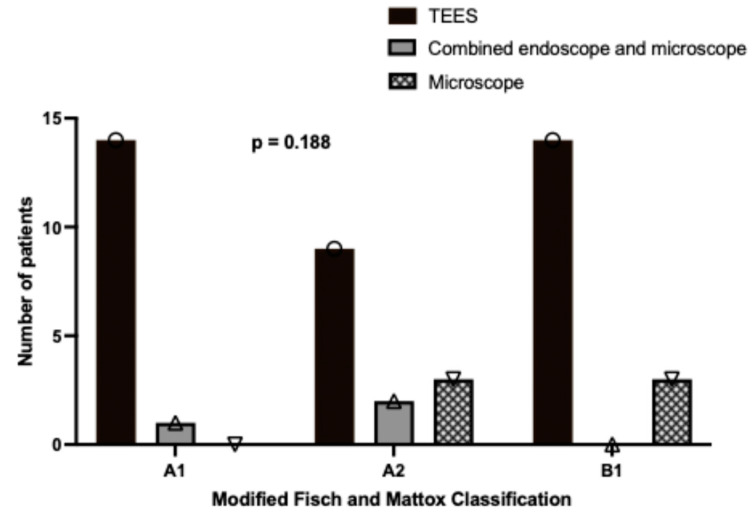
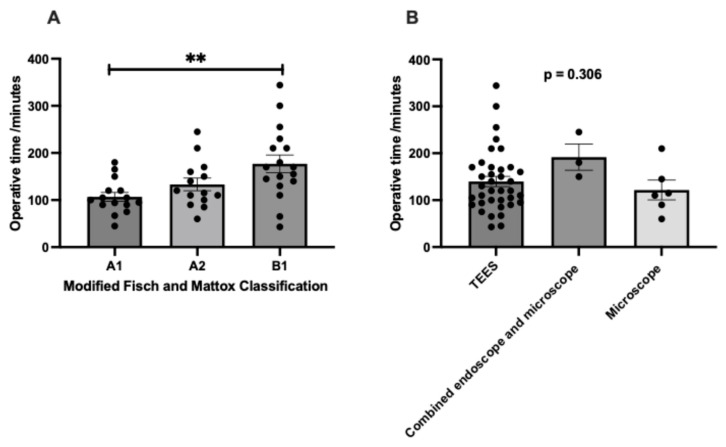
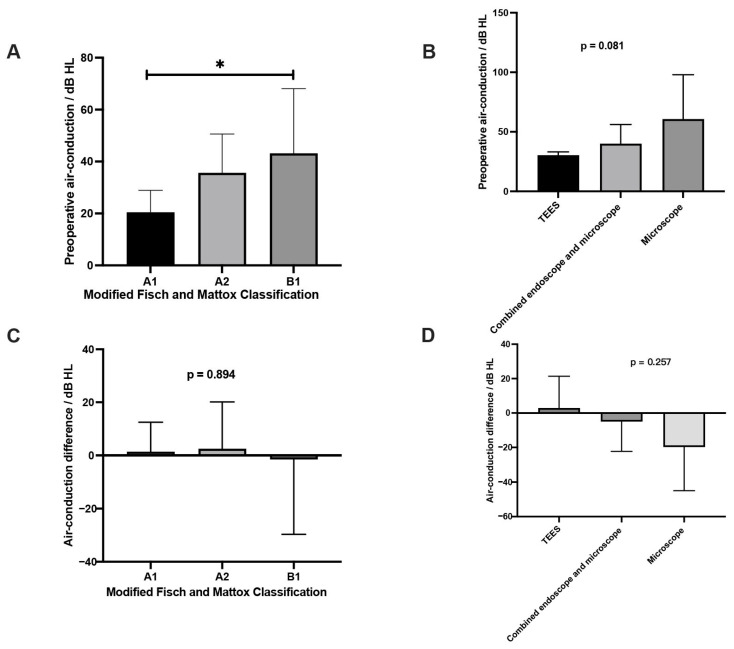
Objective: Comparing the clinical outcomes of glomus tympanicum (GT) resections by transcanal endoscopic ear surgery (TEES), microscopic- and endoscopic-assisted microscopic approaches. Methods: Adult patients conducting exclusive operations for GT within the tympanomastoid cavity were recruited in this retrospective cohort study at five international tertiary referral centers. GT resections were conducted by TEES, microscopic- and endoscopic-assisted microscopic approaches based on modified Fisch-Mattox classifications. Clinical characteristics and surgical outcomes were recorded and analyzed. Results: A total of 46 patients were included. A longer operative time was seen in more advanced GTs (A1: 106.73 ± 9.33 min, A2: 133.21 ± 13.47 min, B1: 176.88 ± 18.69 min, p = 0.005), while no significant differences were observed in the mean operative times among various surgical approaches. Preoperatively, 89.1% of patients experienced pulsatile tinnitus, and 56.5% exhibited conductive hearing loss. Postoperatively, only one patient continued to experience tinnitus (p < 0.001), and two patients had persistent hearing loss (p < 0.001). Higher disease grades correlated with poorer preoperative air-conduction thresholds (p = 0.015), while the differences in air-conduction thresholds before and after surgery did not demonstrate statistical significance across different tumor stages (p = 0.894) and surgical approaches (p = 0.257). The median follow-up period was 4 years, and only one recurrent case was found (2.2%, 1/46), which was treated by TEES and involved a B1 glomus tumor. Conclusions: Similar and excellent surgical outcomes were found among the TEES and microscope- and endoscopic-assisted microscopic approaches in early-stage GTs.
Keywords: endoscopic ear surgery; glomus tympanicum; microscopic surgery; middle ear paraganglioma; transcanal.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Glomus tympanicum removal using transcanal endoscopic assisted surgery: An experience with six cases.World J Otorhinolaryngol Head Neck Surg. 2023 Jul 16;9(4):302-307. doi: 10.1002/wjo2.103. eCollection 2023 Dec. World J Otorhinolaryngol Head Neck Surg. 2023. PMID: 38059144 Free PMC article.
-
Clinical characteristics and surgical strategy of glomus tympanicum tumors.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023 Mar 28;48(3):397-403. doi: 10.11817/j.issn.1672-7347.2023.230206. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 37164923 Free PMC article. Chinese, English.
-
Transcanal Endoscopic Management of Glomus Tympanicum: Multicentric Case Series.Otol Neurotol. 2021 Feb 1;42(2):312-318. doi: 10.1097/MAO.0000000000002929. Otol Neurotol. 2021. PMID: 33351561
-
Endoscopic Management of Glomus Tympanicum Tumor: Report of Three Cases and Review of the Literature.J Audiol Otol. 2023 Jul;27(3):145-152. doi: 10.7874/jao.2022.00276. Epub 2022 Nov 24. J Audiol Otol. 2023. PMID: 36423621 Free PMC article.
-
Current trends and applications in endoscopy for otology and neurotology.World J Otorhinolaryngol Head Neck Surg. 2021 Feb 6;7(2):101-108. doi: 10.1016/j.wjorl.2020.09.003. eCollection 2021 Apr. World J Otorhinolaryngol Head Neck Surg. 2021. PMID: 33997719 Free PMC article. Review.
References
-
- Boedeker C.C., Ridder G.J., Schipper J. Paragangliomas of the head and neck: Diagnosis and treatment. Fam. Cancer. 2005;4:55–59. - PubMed
-
- Fisch U., Mattox D.E. Microsurgery of the Skull Base. George Thieme Verlag; Stuttgart, Germany: 1988.
LinkOut - more resources
Full Text Sources
Miscellaneous
