

Pediatric Preformed Zirconium Oxide Crowns vs. Preformed Metal Crowns After Pulpotomy in Primary Molars: A Practice-Based Retrospective 2.5 Year Cohort Study
- PMID: 40218049
- PMCID: PMC11988542
- DOI: 10.3390/healthcare13070751
Pediatric Preformed Zirconium Oxide Crowns vs. Preformed Metal Crowns After Pulpotomy in Primary Molars: A Practice-Based Retrospective 2.5 Year Cohort Study
Abstract
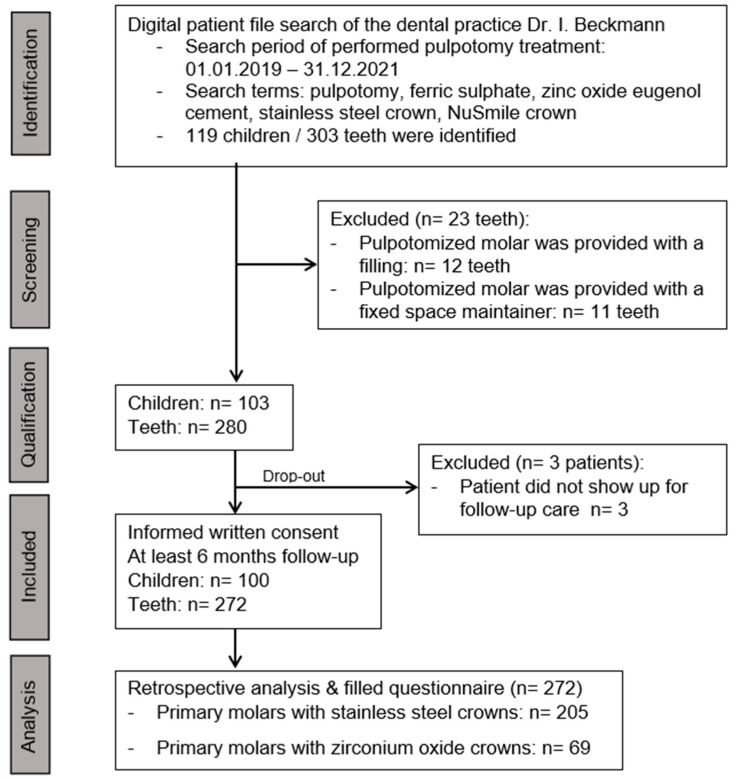
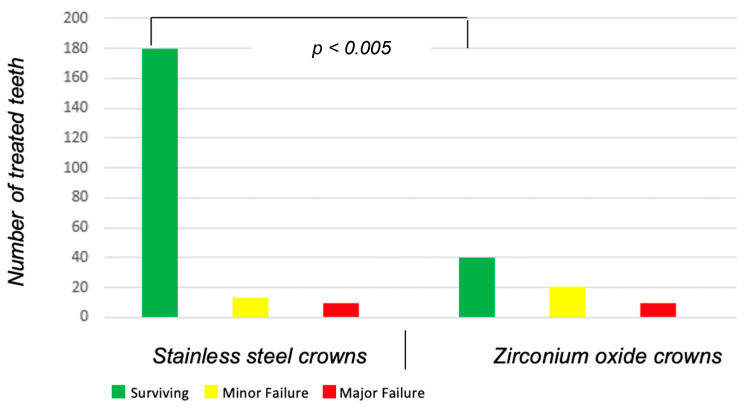
Background: Primary molars with deep carious lesions often require a treatment with pulpotomy and restoration with a crown. Aim: This study aims to compare the survival rates of stainless steel (SSC) and zirconium oxide (ZOC) crowns carried out on pulpotomized primary molars using the International Caries Detection and Assessment System (ICDAS) 4 to 6 lesions. Materials and Methods: The data of 100 patients (mean age 5.3 ± 2.1 years, mean decayed, missing or filled primary teeth (dmft) 7.1 ± 3.2) with 272 primary molars (40, 225, 7 with ICDAS 4, 5, 6, respectively) were collected retrospectively from a specialized private pediatric dental office after ethical approval was obtained and each participant agreed to participation in the study. Primary molars were treated between 2019 and 2021 with pulpotomy (15.5% ferrous sulfate solution for hemostasis and zinc oxide eugenol as a wound dressing) followed by a crown (203 SSC and 69 ZOC) with a minimum follow-up period of 6 months and a mean follow-up time of 28.2 (±11.0) months. Results: Failure occurred significantly less often in SSC (n = 13 out of 203) than in ZOC (n = 20 out of 69; p < 0.001). Major failure was attributed to swelling and abscess (n = 13, 39.4%) followed by the occurrence of fistula (n = 15, 45.4%) and fracture of the crown and abutment (n = 5, 15.2%). Minor failure due to cement dissolution occurred significantly less often in SSC than in ZOC (n = 10 out of 203 vs. n = 9 out of 69; p < 0.005. A Kaplan-Meier survival analysis showed an overall estimated survival time of 38.25 (Confidence interval (CI): 37.0-39.4) months for both types of crowns. A Log-Rank (Mantel-Cox) analysis showed a statistically significant difference (p < 0.05) in the estimated mean survival time of SSC (39.75; CI: 38.5-40.9 months) and ZOC (33.4; CI: 30.5-36.3 months). Survival probability drops just below 80% for ZOC and stays a little over 90% for SCC around the 20th month. Conclusions: SSC showed an advantage over its ZOC counterpart when placed after pulpotomy for the management of primary molars with deep carious lesions. A higher necessity for re-intervention in the more aesthetic ZOC should be considered in clinical decision taking.
Keywords: primary molars; pulpotomy; stainless steel crowns; zirconia crown.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
A clinical and radiographic comparative evaluation of custom-made zirconia crowns using CAD-CAM and stainless steel crowns in primary molars.J Indian Soc Pedod Prev Dent. 2022 Jan-Mar;40(1):34-42. doi: 10.4103/jisppd.jisppd_269_21. J Indian Soc Pedod Prev Dent. 2022. PMID: 35439881
-
Comparison of the treatment outcomes of the conventional stainless steel crown restorations and the hall technique in the treatment of carious primary molars.Niger J Clin Pract. 2021 Apr;24(4):584-594. doi: 10.4103/njcp.njcp_460_20. Niger J Clin Pract. 2021. PMID: 33851682 Clinical Trial.
-
Are pediatric preformed zirconia crowns comparable to preformed metal crowns? A real-life retrospective study.Quintessence Int. 2023 Sep 19;54(8):630-639. doi: 10.3290/j.qi.b4157323. Quintessence Int. 2023. PMID: 37313578
-
The use of stainless steel crowns.Pediatr Dent. 2002 Sep-Oct;24(5):501-5. Pediatr Dent. 2002. PMID: 12412965 Review.
-
Comparison of periodontal health of primary teeth restored with zirconia and stainless steel crowns: A systemic review and meta-analysis.J Formos Med Assoc. 2023 Feb;122(2):148-156. doi: 10.1016/j.jfma.2022.08.015. Epub 2022 Sep 27. J Formos Med Assoc. 2023. PMID: 36180321
References
-
- American Academy of Pediatric Dentistry . The Reference Manual of Pediatric Dentistry. American Academy of Pediatric Dentistry; Chicago, IL, USA: 2023. Pulp therapy for primary and immature permanent teeth.
-
- Farooq N.S., Coll J.A., Kuwabara A., Shelton P. Success rates of formocresol pulpotomy and indirect pulp therapy in the treatment of deep dentinal caries in primary teeth. Pediatr. Dent. 2000;22:278–286. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
