

The Evaluation, Diagnosis, and Management of Ovarian Cysts, Masses, and Their Complications in Fetuses, Infants, Children, and Adolescents
- PMID: 40218072
- PMCID: PMC11988711
- DOI: 10.3390/healthcare13070775
The Evaluation, Diagnosis, and Management of Ovarian Cysts, Masses, and Their Complications in Fetuses, Infants, Children, and Adolescents
Abstract
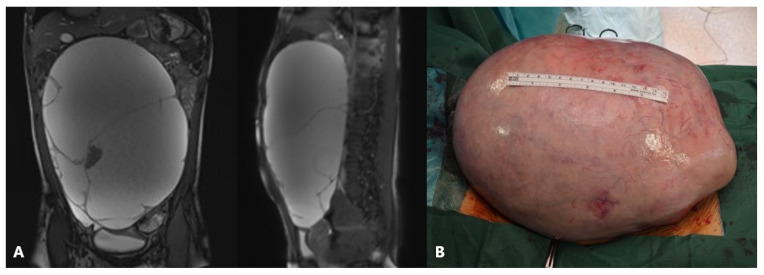
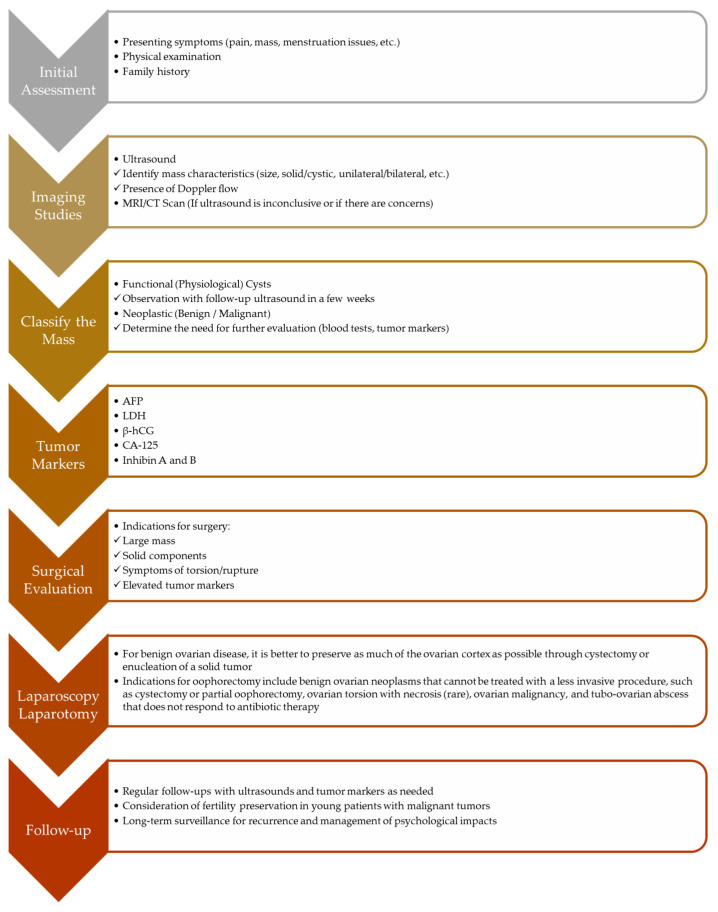
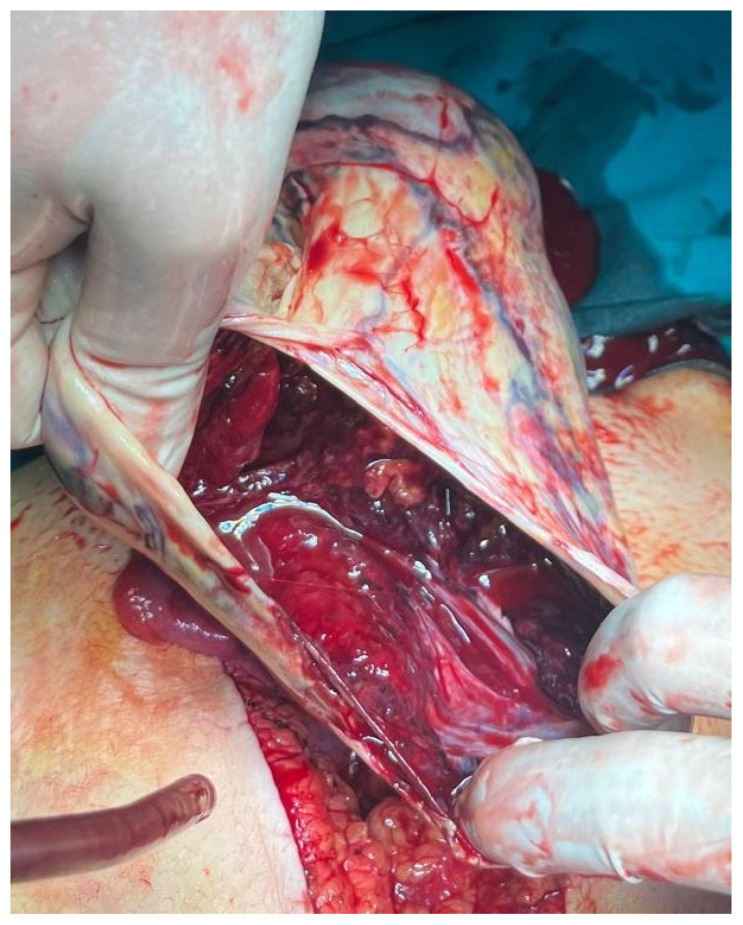
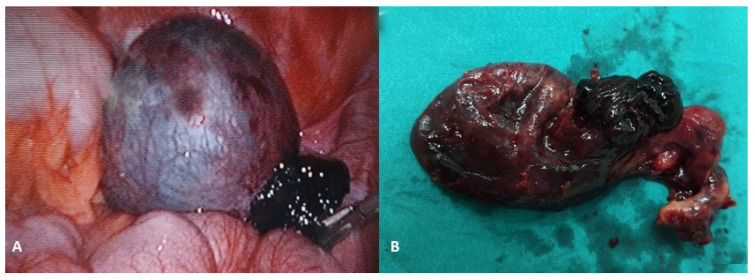
The majority of abdominal masses in female children derive from the ovaries. Ovarian masses in pediatric populations can vary from simple functional cysts to malignant neoplasms. Their incidence, clinical presentation, and histological distribution vary across age groups. In the assessment of ovarian masses in children, the primary aim is to determine the probability of malignancy, as the treatment approaches for benign and malignant lesions are significantly distinct. The primary imaging tool for evaluating ovarian cysts and masses is ultrasound, which can assess the size, location, and characteristics of masses. Magnetic resonance imaging (MRI) or computed tomography (CT) may be used for further evaluation if ultrasound findings are inconclusive or if malignancy is suspected, especially in older adolescents. Serum markers may be considered in older adolescents to help assess the risk of malignancy, though it is less useful in younger populations due to normal developmental variations. Many functional ovarian cysts, especially those detected in fetuses or infants, often resolve spontaneously without intervention. Surgical intervention is indicated in cases of large cysts that cause symptoms, or if there are concerns for malignancy. Common procedures include primarily ovarian sparing laparoscopy or laparotomy. Complications like torsion, rupture, or hemorrhage may require urgent surgical intervention. Treatment should be performed in specialized centers to avoid unnecessary oophorectomies and ensure the best possible outcome for the patient. This comprehensive review aims to provide an overview of the evaluation, diagnosis, and treatment of ovarian masses in the pediatric population. Emphasis is placed on the particularities of the lesions and their management in relation to age subgroups.
Keywords: adolescent; children; cystectomy; fetus; gynecology; infant; oophorectomy; ovarian cyst; ovarian mass; ovary; pediatric surgery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Ovarian Masses in Children and Adolescents: A Review of the Literature with Emphasis on the Diagnostic Approach.Children (Basel). 2023 Jun 27;10(7):1114. doi: 10.3390/children10071114. Children (Basel). 2023. PMID: 37508611 Free PMC article. Review.
-
Review of a 25-Year Experience in the Management of Ovarian Masses in Neonates, Children and Adolescents: From Laparoscopy to Robotics and Indocyanine Green Fluorescence Technology.Children (Basel). 2022 Aug 12;9(8):1219. doi: 10.3390/children9081219. Children (Basel). 2022. PMID: 36010109 Free PMC article. Review.
-
Surgical Management of Adnexal Masses in the Pediatric and Adolescent Age Group: Our Experience.J Indian Assoc Pediatr Surg. 2021 Sep-Oct;26(5):287-293. doi: 10.4103/jiaps.JIAPS_136_20. Epub 2021 Sep 16. J Indian Assoc Pediatr Surg. 2021. PMID: 34728912 Free PMC article.
-
Ovarian masses in children and adolescents - an analysis of 521 clinical cases.J Pediatr Adolesc Gynecol. 2014 Jun;27(3):e73-7. doi: 10.1016/j.jpag.2013.07.007. Epub 2013 Oct 21. J Pediatr Adolesc Gynecol. 2014. PMID: 24157281
-
Ovarian masses in young adolescents: imaging findings with surgical confirmation.Eur J Gynaecol Oncol. 2004;25(2):201-6. Eur J Gynaecol Oncol. 2004. PMID: 15032282
Cited by
-
Imaging Evaluation of Ovarian Masses in a Pediatric Population: A Comprehensive Overview.Cancers (Basel). 2025 Jul 11;17(14):2316. doi: 10.3390/cancers17142316. Cancers (Basel). 2025. PMID: 40723200 Free PMC article. Review.
References
-
- Ciro E., Vincenzo C., Mariapina C., Fulvia D.C., Vincenzo B., Giorgia E., Roberto C., Lepore B., Castagnetti M., Califano G., et al. Review of a 25-Year Experience in the Management of Ovarian Masses in Neonates, Children and Adolescents: From Laparoscopy to Robotics and Indocyanine Green Fluorescence Technology. Children. 2022;9:1219. doi: 10.3390/children9081219. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
