

Acylcarnitine and Free Fatty Acid Profiles in Primary Biliary Cholangitis: Associations with Fibrosis and Inflammation
- PMID: 40218855
- PMCID: PMC11990100
- DOI: 10.3390/nu17071097
Acylcarnitine and Free Fatty Acid Profiles in Primary Biliary Cholangitis: Associations with Fibrosis and Inflammation
Abstract
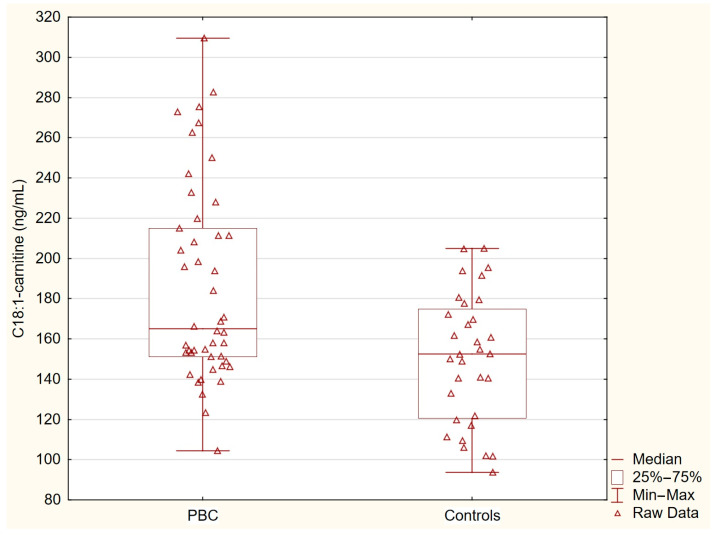
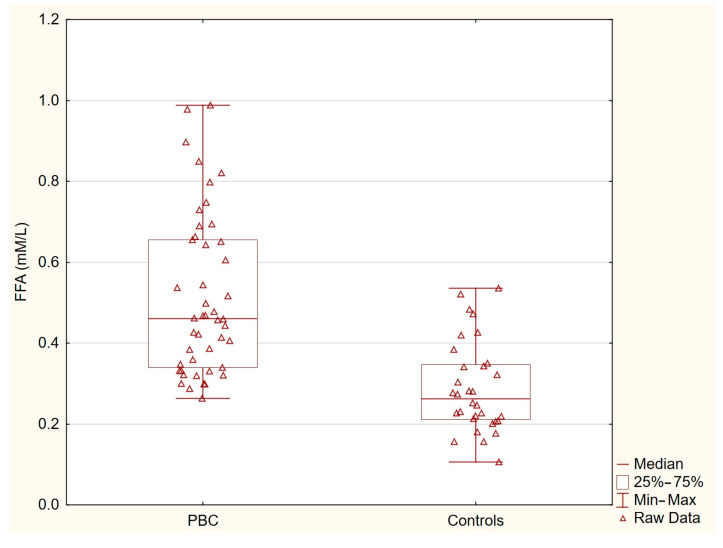
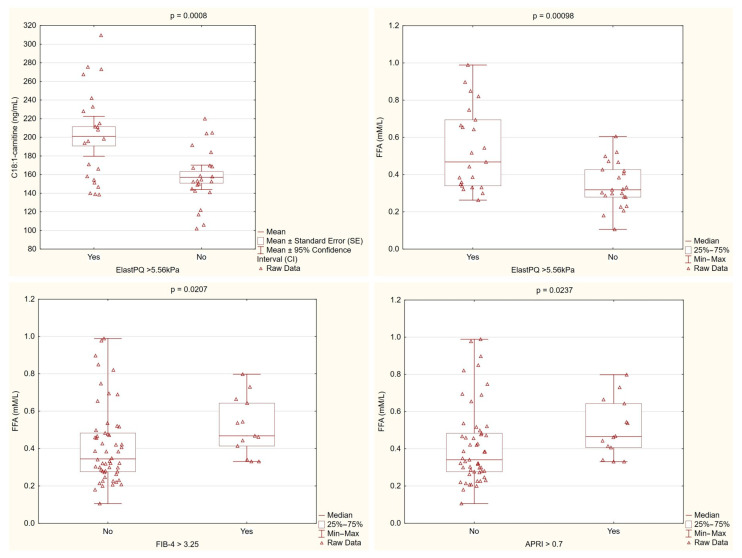
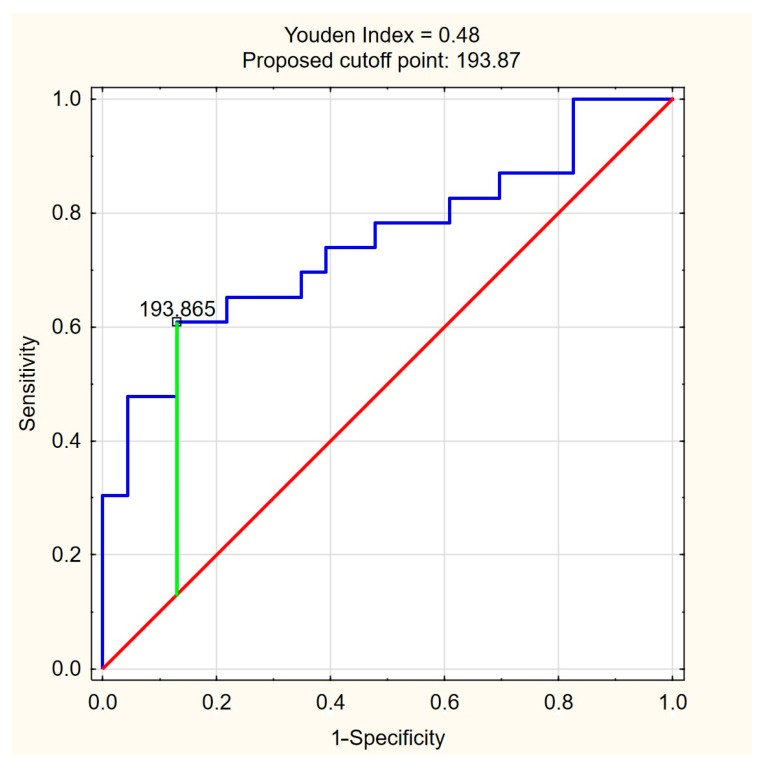
Background: Primary biliary cholangitis (PBC) is a chronic autoimmune liver disease characterized by bile duct destruction, cholestasis, and fibrosis. Acylcarnitines are esters of carnitine responsible for the transport of long-chain fatty acids into mitochondria for β-oxidation, playing a crucial role in energy metabolism and lipid homeostasis. This study aimed to assess acylcarnitine and free fatty acid (FFA) profiles in PBC patients and their associations with fibrosis severity and inflammation. Methods: This cross-sectional study included 46 PBC patients and 32 healthy controls. Acylcarnitines and FFAs were quantified using liquid chromatography-tandem mass spectrometry (LC-MS/MS) and enzymatic assays, respectively. Liver stiffness was measured by point shear wave elastography (ElastPQ), and fibrosis was assessed using APRI and FIB-4 scores. Inflammatory markers (IL-6, IL-1β) were also analyzed. Results: PBC patients had significantly higher levels of C18:1-acylcarnitine (median: 165.1 ng/mL) compared with the controls (152.4 ng/mL, p = 0.0036). Similarly, the FFA levels were markedly elevated in the PBC patients (median: 0.46 mM/L) compared with the controls (0.26 mM/L, p < 0.0001). Patients with higher liver stiffness (ElastPQ > 5.56 kPa) had significantly elevated C18:1-acylcarnitine (p = 0.0008) and FFA levels (p = 0.00098). Additionally, FFAs were significantly increased in patients with higher APRI and FIB-4 scores and were associated with elevated inflammatory markers (IL-6, IL-1β) and liver injury markers. Multivariate regression analysis confirmed C18:1-acylcarnitine (OR = 1.031, 95% CI: 1.007-1.057, p = 0.013) and FFAs (OR = 2.25 per 0.1 mM/L increase, 95% CI: 1.20-4.22, p = 0.012) as independent predictors of fibrosis severity in PBC. Conclusions: C18:1-acylcarnitine and FFAs are significantly elevated in PBC and are strongly associated with fibrosis severity and inflammation. These findings suggest a link between lipid metabolism disturbances and PBC. Both metabolites may potentially serve as non-invasive biomarkers of fibrosis progression in PBC, warranting further investigation.
Keywords: acylcarnitines; bile acids; fibrosis; free fatty acids; inflammation; liver stiffness; metabolic biomarkers; mitochondrial dysfunction; primary biliary cholangitis; β-oxidation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Diagnostic performance of a point shear wave elastography (pSWE) for hepatic fibrosis in patients with autoimmune liver disease.PLoS One. 2019 Mar 11;14(3):e0212771. doi: 10.1371/journal.pone.0212771. eCollection 2019. PLoS One. 2019. PMID: 30856201 Free PMC article. Clinical Trial.
-
Elevated Plasma BDNF in Early Primary Biliary Cholangitis: Associations with Liver Fibrosis, IL-6, IL-18, Fatigue, and Cognitive Impairment.Int J Mol Sci. 2025 Jul 24;26(15):7142. doi: 10.3390/ijms26157142. Int J Mol Sci. 2025. PMID: 40806277 Free PMC article.
-
Minimal hepatic encephalopathy may be present despite the absence of non-invasive and elastography evidence of cirrhosis in patients with primary biliary cholangitis.Adv Med Sci. 2021 Sep;66(2):293-301. doi: 10.1016/j.advms.2021.06.001. Epub 2021 Jun 27. Adv Med Sci. 2021. PMID: 34192643
-
Diagnostic accuracy of vibration-controlled transient elastography for staging liver fibrosis in autoimmune liver diseases: A systematic review and meta-analysis.Clin Mol Hepatol. 2024 Sep;30(Suppl):S134-S146. doi: 10.3350/cmh.2024.0586. Epub 2024 Aug 21. Clin Mol Hepatol. 2024. PMID: 39165158 Free PMC article.
-
Systematic review and meta-analysis: Transient elastography compared to liver biopsy for staging of liver fibrosis in primary biliary cholangitis.Ann Hepatol. 2023 Jul-Aug;28(4):101107. doi: 10.1016/j.aohep.2023.101107. Epub 2023 Apr 23. Ann Hepatol. 2023. PMID: 37088420
Cited by
-
Migratory and intermittent polyarthritis as an atypical presentation of carnitine palmitoyltransferase II deficiency with positive response to treatment with Interleukin-1 receptor antagonist: a case presentation and case-based review.Rheumatol Int. 2025 Jun 28;45(7):161. doi: 10.1007/s00296-025-05917-0. Rheumatol Int. 2025. PMID: 40580346 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
