

High-Density Lipoprotein Particles, Inflammation, and Coronary Heart Disease Risk
- PMID: 40218941
- PMCID: PMC11990870
- DOI: 10.3390/nu17071182
High-Density Lipoprotein Particles, Inflammation, and Coronary Heart Disease Risk
Abstract
Background: Coronary heart disease (CHD) remains a leading cause of death and has been associated with alterations in plasma lipoprotein particles and inflammation markers. This study aimed to evaluate and compare standard and advanced lipid parameters and inflammatory biomarkers in CHD cases and matched control subjects. We hypothesized that incorporating advanced lipid and inflammatory biomarkers into risk models would improve CHD risk prediction beyond the standard lipid measures.
Methods: CHD cases (n = 227, mean age 61 years, 47% female) and matched controls (n = 526) underwent fasting blood collection while off lipid-lowering medications. Automated chemistry analyses were performed to measure total cholesterol (TC), triglycerides (TGs), low-density lipoprotein-C (LDL-C), small dense LDL-C (sdLDL-C), apolipoproteins (apos) A-I and B, lipoprotein(a) (Lp(a)), high-sensitivity C-reactive protein (hsCRP), serum amyloid-A (SAA), myeloperoxidase (MPO), and apoA-I in HDL particles (via 2-dimensional electrophoresis and immunoblotting). Univariate, multivariate, and machine learning analyses compared the CHD cases with the controls.
Results: The most significant percent differences between male and female cases versus controls were for hsCRP (+78%, +200%), MPO (+109%, +106%), SAA (+84%, +33%), sdLDL-C (+48%; +43%), Lp(a) (+43%,+70%), apoA-I in very large α-1 HDL (-34%, -26%), HDL-C (-24%, -27%), and apoA-I in very small preβ-1 HDL (+17%; +16%). Total C, non-HDL-C, and direct and calculated LDL-C levels were only modestly higher in the cases. Multivariate models incorporating advanced parameters were statistically superior to a standard model (C statistic: men: 0.913 vs. 0.856; women: 0.903 versus 0.838). Machine learning identified apoA-I in preβ-1-HDL, α-2-HDL, α-1-HDL, α-3-HDL, MPO, and sdLDL-C as the top predictors of CHD.
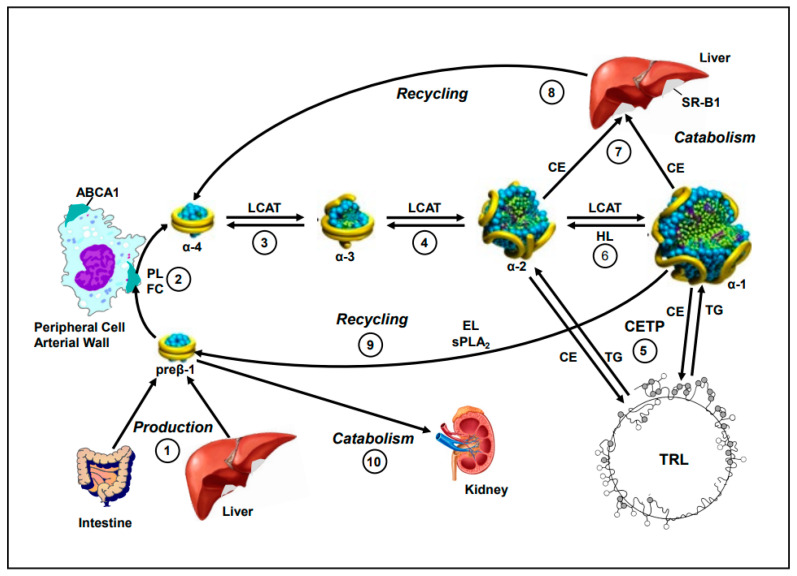
Conclusions: This study introduces a novel approach to CHD risk assessment by integrating advanced HDL particle analysis and machine learning. By assessing HDL subpopulations (α-1, α-2, preβ-1 HDL), inflammatory biomarkers (MPO, SAA), and small dense LDL, we provide a more refined stratification model. Notably, preβ-1 HDL, an independent risk factor reflecting impaired cholesterol efflux from the artery wall, is highlighted as a critical marker of CHD risk. Our approach allows for earlier identification of high-risk individuals, particularly those with subtle lipid or inflammatory abnormalities, supporting more personalized interventions. These findings demonstrate the potential of advanced lipid profiling and machine learning to enhance CHD risk prediction.
Keywords: CHD; HDL; inflammation.
Conflict of interest statement
John P. Kane, has received research grants (to the University of California San Francisco) from Boston Heart Diagnostics (Framingham, MA). He, Diffenderfer, Asztalos are current or past employees of Boston Heart Diagnostics (Framingham, MA). All other authors do not have relevant relationships or conflicts of interest to disclose.
Figures
References
-
- Khan S.S., Matsushita K., Sang Y., Ballew S.H., Grams M.E., Surapaneni A., Blaha M.J., Carson A.P., Chang A.R., Ciemins E., et al. Development and Validation of the American Heart Association’s PREVENT Equations. Circulation. 2024;149:430–449. doi: 10.1161/CIRCULATIONAHA.123.067626. Erratum in Circulation 2024, 149, e956. https://doi.org/10.1161/CIR.0000000000001230 . - DOI - PMC - PubMed
-
- Khan S.S., Coresh J., Pencina M.J., Ndumele C.E., Rangaswami J., Chow S.L., Palaniappan L.P., Sperling L.S., Virani S.S., Ho J.E., et al. Novel Prediction Equations for Absolute Risk Assessment of Total Cardiovascular Disease Incorporating Cardiovascular-Kidney-Metabolic Health: A Scientific Statement from the American Heart Association. Circulation. 2023;148:1982–2004. doi: 10.1161/CIR.0000000000001191. - DOI - PubMed
-
- GGrundy S.M., Stone N.J., Bailey A.L., Beam C., Birtcher K.K., Blumenthal R.S., Braun L.T., de Ferranti S., Faiella-Tommasino J., Forman D.E., et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082–e1143. doi: 10.1161/CIR.0000000000000625. Erratum in Circulation 2019, 139, e1182–e1186. https://doi.org/10.1161/CIR.0000000000000698 . Erratum in Circulation 2023, 148, e5. https://doi.org/10.1161/CIR.0000000000001172 . - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
