

Federated learning with multi-cohort real-world data for predicting the progression from mild cognitive impairment to Alzheimer's disease
- PMID: 40219846
- PMCID: PMC11992589
- DOI: 10.1002/alz.70128
Federated learning with multi-cohort real-world data for predicting the progression from mild cognitive impairment to Alzheimer's disease
Abstract
Introduction: Leveraging routinely collected electronic health records (EHRs) from multiple health-care institutions, this approach aims to assess the feasibility of using federated learning (FL) to predict the progression from mild cognitive impairment (MCI) to Alzheimer's disease (AD).
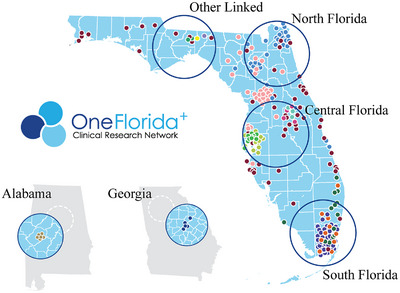
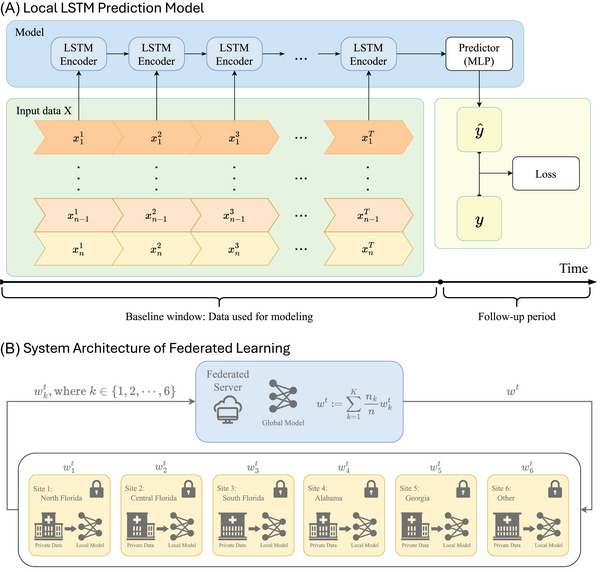
Methods: We analyzed EHR data from the OneFlorida+ consortium, simulating six sites, and used a long short-term memory (LSTM) model with a federated averaging (FedAvg) algorithm. A personalized FL approach was used to address between-site heterogeneity. Model performance was assessed using the area under the receiver operating characteristic curve (AUC) and feature importance techniques.
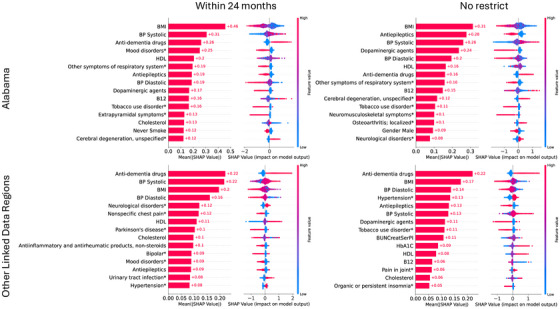
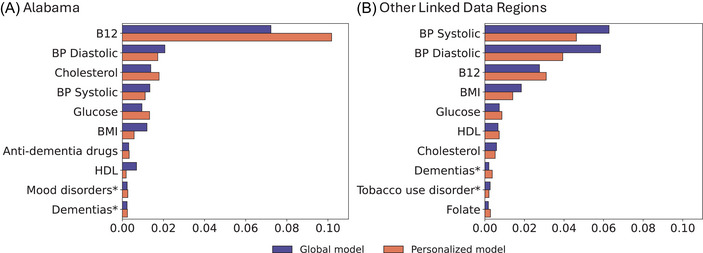
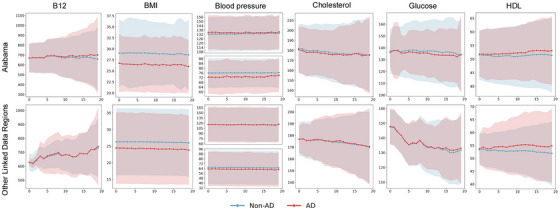
Results: Of 44,899 MCI patients, 6391 progressed to AD. FL models achieved a 6% improvement in AUC compared to local models. Key predictive features included body mass index, vitamin B12, blood pressure, and others.
Discussion: FL showed promise in predicting AD progression by integrating heterogeneous data across multiple institutions while preserving privacy. Despite limitations, it offers potential for future clinical applications.
Highlights: We applied long short-term memory and federated learning (FL) to predict mild cognitive impairment to Alzheimer's disease progression using electronic health record data from multiple institutions. FL improved prediction performance, with a 6% increase in area under the receiver operating characteristic curve compared to local models. We identified key predictive features, such as body mass index, vitamin B12, and blood pressure. FL shows effectiveness in handling data heterogeneity across multiple sites while ensuring data privacy. Personalized and pooled FL models generally performed better than global and local models.
Keywords: Alzheimer's disease; federated learning; long short‐term memory; mild cognitive impairment.
© 2025 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors declare no competing interests. Author disclosures are available in the supporting information.
Figures
Similar articles
-
Graph Convolutional Network for AD and MCI Diagnosis Utilizing Peripheral DNA Methylation: Réseau de neurones en graphes pour le diagnostic de la MA et du TCL à l'aide de la méthylation de l'ADN périphérique.Can J Psychiatry. 2024 Dec;69(12):869-879. doi: 10.1177/07067437241300947. Epub 2024 Nov 25. Can J Psychiatry. 2024. PMID: 39584743 Free PMC article.
-
Predicting progression from mild cognitive impairment to Alzheimer's disease on an individual subject basis by applying the CARE index across different independent cohorts.Aging (Albany NY). 2019 Apr 30;11(8):2185-2201. doi: 10.18632/aging.101883. Aging (Albany NY). 2019. PMID: 31078129 Free PMC article.
-
ApoE4 effects on automated diagnostic classifiers for mild cognitive impairment and Alzheimer's disease.Neuroimage Clin. 2014 Jan 4;4:461-72. doi: 10.1016/j.nicl.2013.12.012. eCollection 2014. Neuroimage Clin. 2014. PMID: 24634832 Free PMC article.
-
Structural magnetic resonance imaging for the early diagnosis of dementia due to Alzheimer's disease in people with mild cognitive impairment.Cochrane Database Syst Rev. 2020 Mar 2;3(3):CD009628. doi: 10.1002/14651858.CD009628.pub2. Cochrane Database Syst Rev. 2020. PMID: 32119112 Free PMC article.
-
Privacy-preserving federated data access and federated learning: Improved data sharing and AI model development in transfusion medicine.Transfusion. 2025 Jan;65(1):22-28. doi: 10.1111/trf.18077. Epub 2024 Nov 29. Transfusion. 2025. PMID: 39610333 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
