

Impact of hypertension on cerebral small vessel disease: A post-mortem study of microvascular pathology from normal-appearing white matter into white matter hyperintensities
- PMID: 40219923
- PMCID: PMC11994636
- DOI: 10.1177/0271678X251333256
Impact of hypertension on cerebral small vessel disease: A post-mortem study of microvascular pathology from normal-appearing white matter into white matter hyperintensities
Abstract
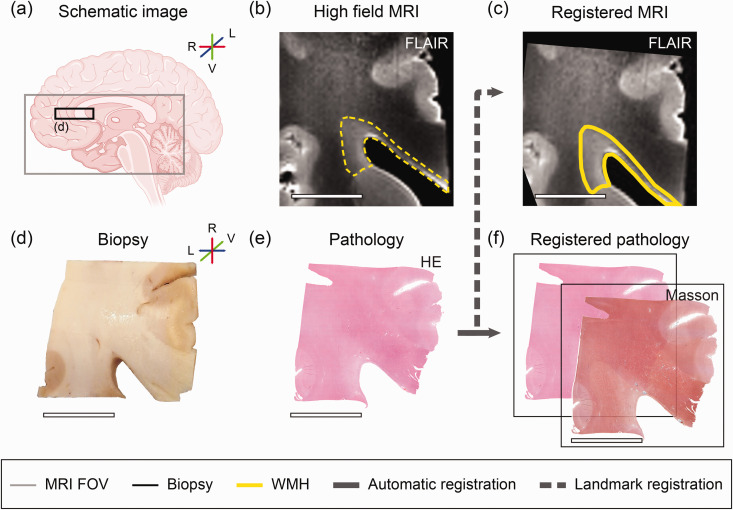
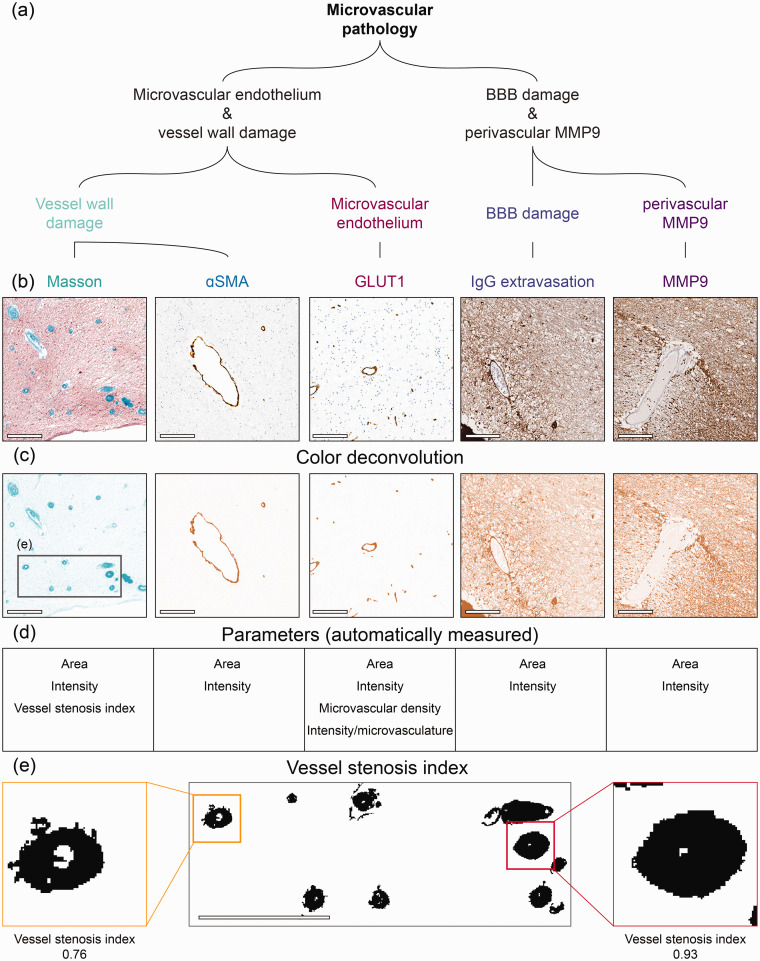
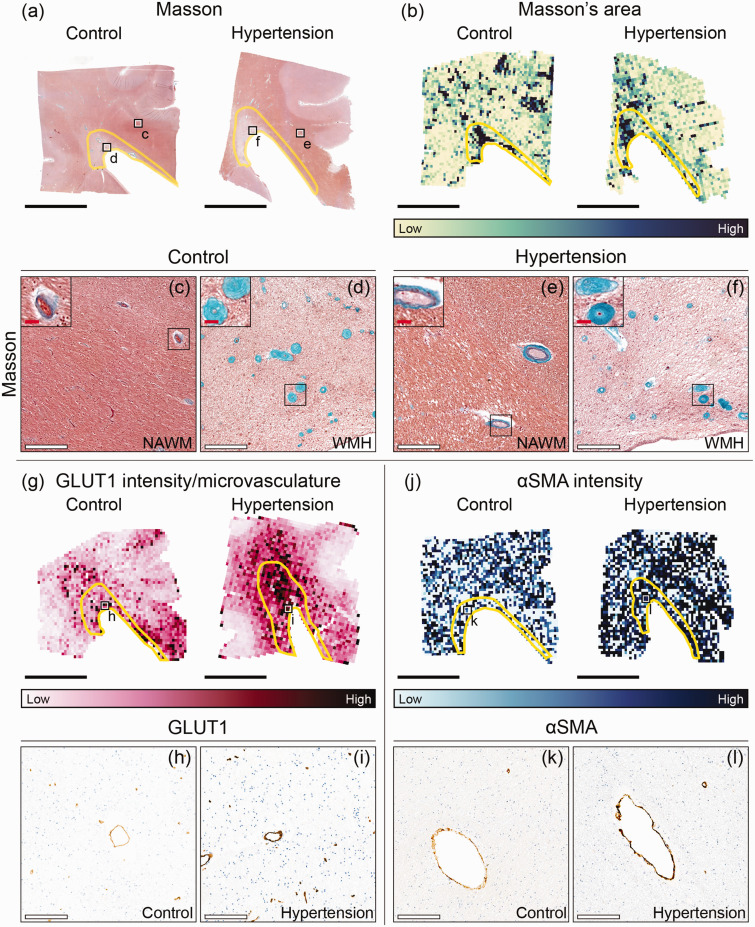
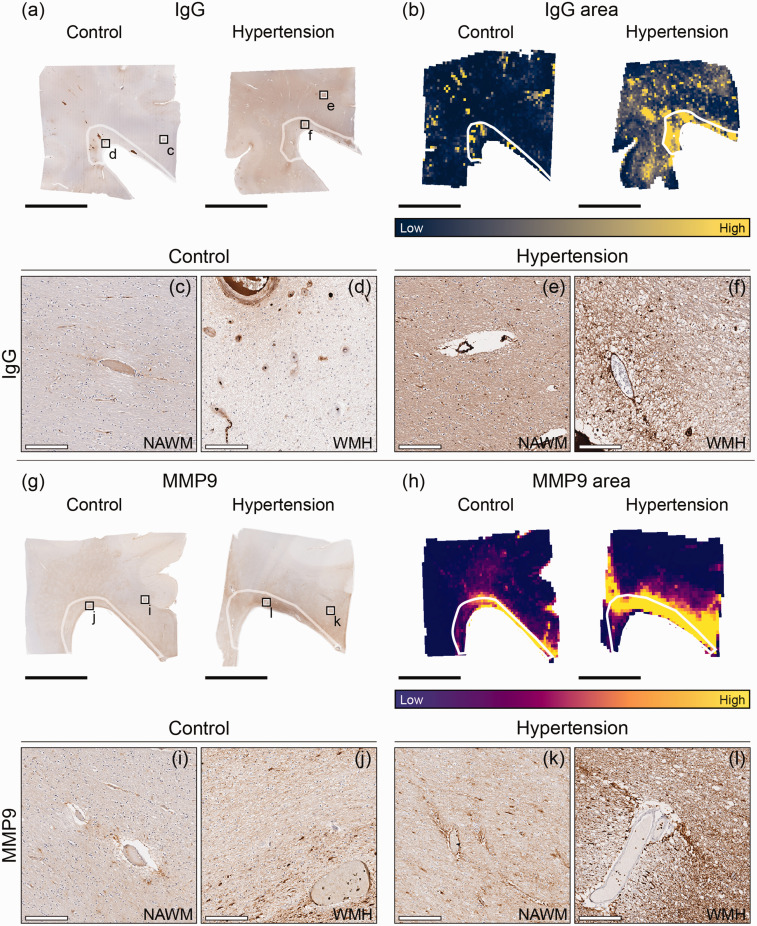
Cerebral small vessel disease (SVD) is diagnosed through imaging hallmarks like white matter hyperintensities (WMH). Novel hypotheses imply that endothelial dysfunction, blood-brain barrier (BBB) disruption and neurovascular inflammation contribute to conversion of normal-appearing white matter (NAWM) into WMH in hypertensive individuals. Aiming to unravel the association between chronic hypertension and the earliest WMH pathogenesis, we characterized microvascular pathology in periventricular NAWM into WMH in post-mortem brains of individuals with and without hypertension. Our second aim was to delineate the NAWM-WMH transition from NAWM towards the center of WMH using deep learning, refining WMH segmentation capturing increases in FLAIR signal. Finally, we aimed to demonstrate whether these processes may synergistically contribute to WMH pathogenesis by performing voxel-wise correlations between MRI and microvascular pathology. Larger endothelium disruption, BBB damage and neurovascular inflammation were observed in individuals with hypertension. We did not observe gradual BBB damage nor neurovascular inflammation along the NAWM-WMH transition. We found a strong correlation between BBB damage and neurovascular inflammation in all individuals in both periventricular NAWM and WMH. These novel findings suggest that endothelium disruption, BBB damage and neurovascular inflammation are major contributors to SVD progression, but being already present in NAWM in hypertension.
Keywords: Blood-brain barrier; MRI; hypertension; immunohistochemistry; inflammation; neuropathology; small vessel disease.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol 2019; 18: 684–696. - PubMed
-
- Hilal S, Mok V, Youn YC, et al. Prevalence, risk factors and consequences of cerebral small vessel diseases: data from three Asian countries. J Neurol Neurosurg Psychiatry 2017; 88: 669–674. - PubMed
-
- Pantoni L. Cerebral small vessel disease from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 2010; 9: 689–701. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
