

Predictive scoring systems for mortality in heart transplant patients with liver cirrhosis
- PMID: 40221468
- PMCID: PMC11993772
- DOI: 10.1038/s41598-025-87675-4
Predictive scoring systems for mortality in heart transplant patients with liver cirrhosis
Abstract
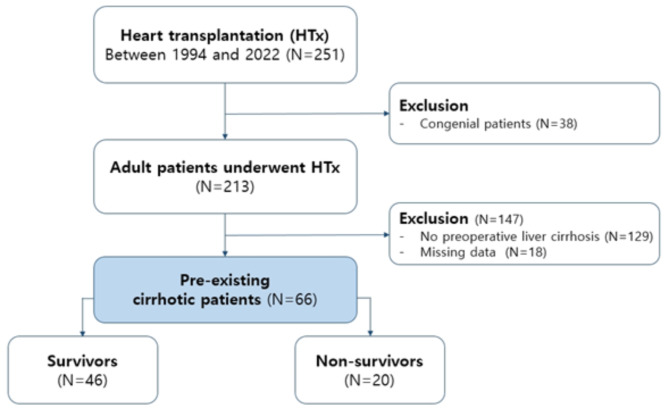
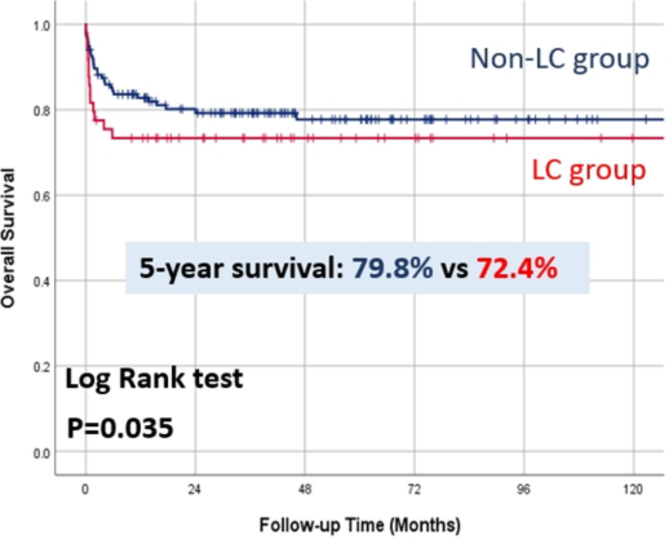
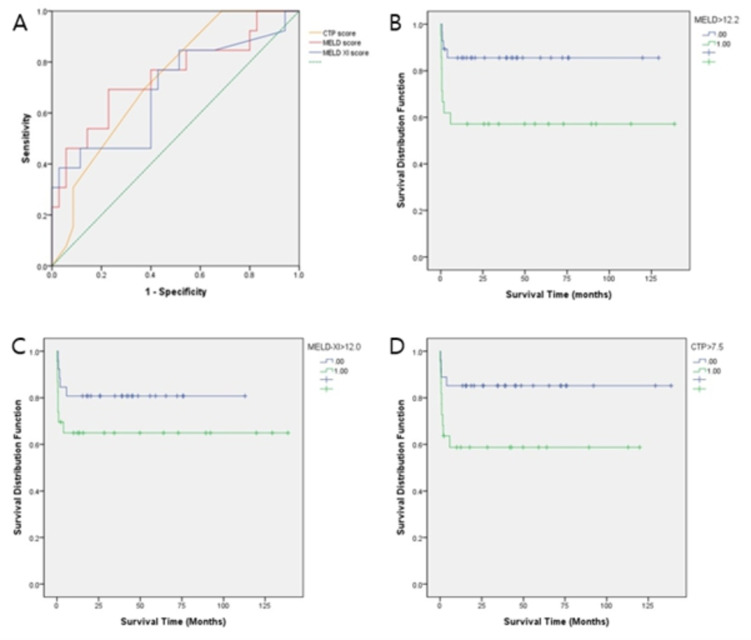
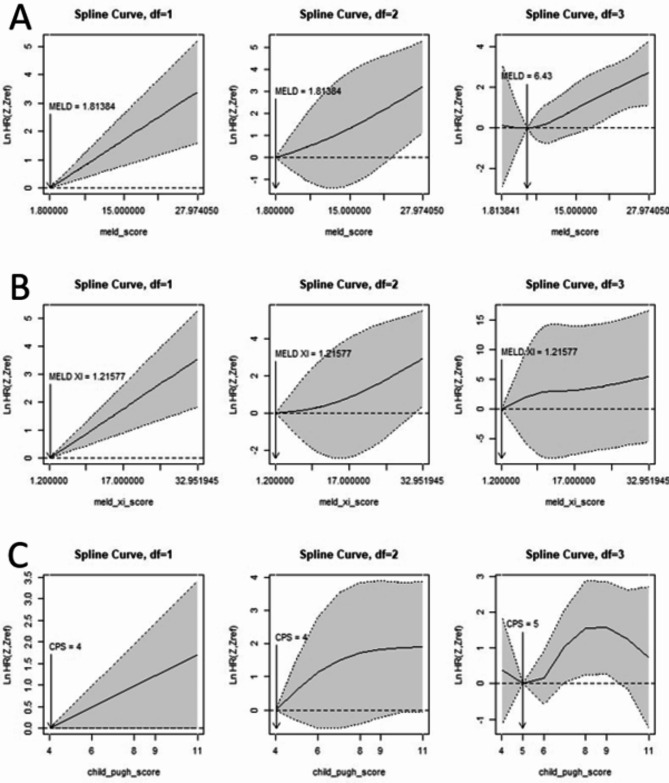
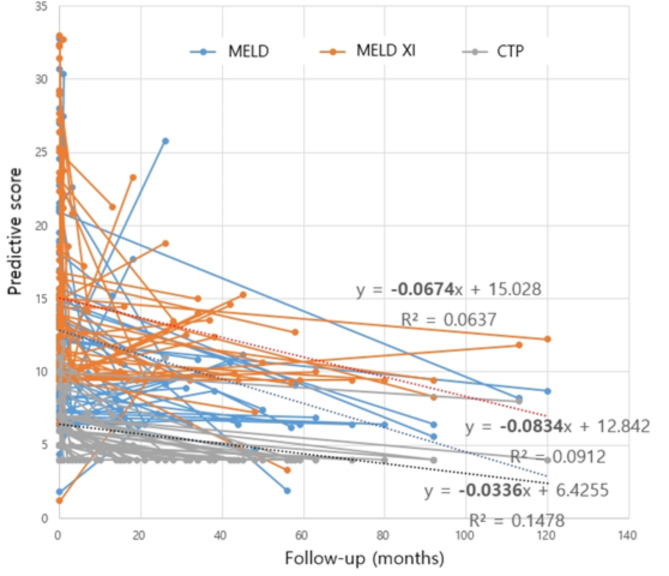
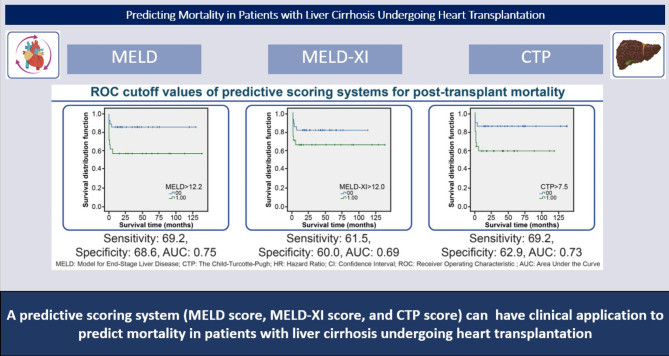
To compare the Model for End-Stage Liver Disease (MELD), MELD-XI, and Child-Turcotte-Pugh (CTP) scores for risk prediction in patients with cirrhosis undergoing heart transplantation. This study enrolled 66 consecutive patients (26 males; median age, 46 [18-68] years) with liver cirrhosis who underwent heart transplantation at our institution from 1994 to 2022. Potential preoperative outcome predictors and the preoperative MELD, MELD-XI, and CTP scores were calculated. The median follow-up duration was 45.2 months. The MELD (p = 0.01) and MELD-XI scores (p < 0.01) were significantly different between survivors and non-survivors. Cox regression analysis showed that high MELD (hazard ratio [HR] 1.07; 95% confidence interval [CI], 1.03-1.11; p < 0.01), MELD-XI (HR, 1.16; 95% CI, 1.06-1.21; p < 0.01), and CTP scores (HR, 1.43; 95% CI, 1.20-1.75; p = 0.01) were associated with the risk of all-cause mortality. Receiver operating characteristic curve analysis revealed that the optimal cut-off values of MELD, MELD-XI, and CTP scores were 12.2, 12.0, and 7.5, respectively (sensitivity: 69.2, 61.5, and 69.2%; specificity: 68.6, 60.0, and 62.9%, respectively) for all-cause mortality (area under the curve: 0.75, 0.69, and 0.73, respectively). Patients with advanced heart failure and liver cirrhosis have high mortality and morbidity rates after heart transplantation. However, these scoring systems can be used as risk stratification tools in patients with liver cirrhosis undergoing heart transplantation.Research registration unique identifying number: Research Registry (UIN: resarchregistry10791).
Keywords: Heart transplantation; Liver cirrhosis; Liver failure.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Integrated model for end-stage liver disease maybe superior to some other model for end-stage liver disease-based systems in addition to Child-Turcotte-Pugh and albumin-bilirubin scores in patients with hepatitis B virus-related liver cirrhosis and spontaneous bacterial peritonitis.Eur J Gastroenterol Hepatol. 2019 Oct;31(10):1256-1263. doi: 10.1097/MEG.0000000000001481. Eur J Gastroenterol Hepatol. 2019. PMID: 31498284
-
Child-Turcotte-Pugh versus MELD-XI identify distinct high-risk populations for heart transplantation following ventricular assist device placement.Clin Transplant. 2022 May;36(5):e14617. doi: 10.1111/ctr.14617. Epub 2022 Feb 26. Clin Transplant. 2022. PMID: 35191097
-
Predictive Value of the Model for End-Stage Liver Disease Score Excluding International Normalized Ratio One Year After Orthotopic Heart Transplantation.Transplant Proc. 2016 Jun;48(5):1703-7. doi: 10.1016/j.transproceed.2015.12.136. Transplant Proc. 2016. PMID: 27496475
-
Predictors of mortality in cirrhotic patients undergoing extrahepatic surgery: comparison of Child-Turcotte-Pugh and model for end-stage liver disease-based indices.ANZ J Surg. 2014 Nov;84(11):832-6. doi: 10.1111/ans.12198. Epub 2013 May 6. ANZ J Surg. 2014. PMID: 23647879
-
Preoperative hepatic dysfunction could predict postoperative mortality and morbidity in patients undergoing cardiac surgery: Utilization of the MELD scoring system.Int J Cardiol. 2016 Jan 15;203:682-9. doi: 10.1016/j.ijcard.2015.10.181. Epub 2015 Oct 26. Int J Cardiol. 2016. PMID: 26583843
References
-
- Hosenpud, J. D., Bennett, L. E., Keck, B. M., Boucek, M. M. & Novick, R. J. The Registry of the International Society for Heart and Lung Transplantation: 18th official report 2001. J. Heart Lung Transpl.20 (8), 805–815 (2001). - PubMed
-
- Kobashigawa, J. et al. Report from the American Society of Transplantation Conference on donor heart selection in adult cardiac transplantation in the United States. Am. J. Transpl.17 (10), 2559–2566 (2017). - PubMed
-
- Slaughter, M. S. Long-term continuous flow left ventricular assist device support and end-organ function: Prospects for destination therapy. J. Cardiothorac. Surg.25 (4), 490–494 (2010). - PubMed
-
- Kamdar, F. et al. Effects of centrifugal, axial and pulsatile left ventricular assist device support on end-organ function in heart failure patients. J. Heart Lung Transpl.28 (4), 352–359 (2009). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
