

The clinical frailty scale improves risk prediction in older emergency department patients: a comparison with qSOFA, NEWS2, and REMS
- PMID: 40221594
- PMCID: PMC11993572
- DOI: 10.1038/s41598-025-97764-z
The clinical frailty scale improves risk prediction in older emergency department patients: a comparison with qSOFA, NEWS2, and REMS
Abstract
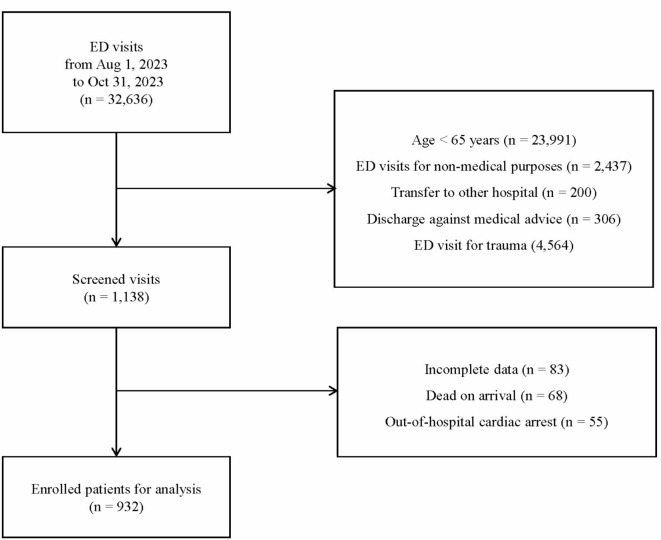
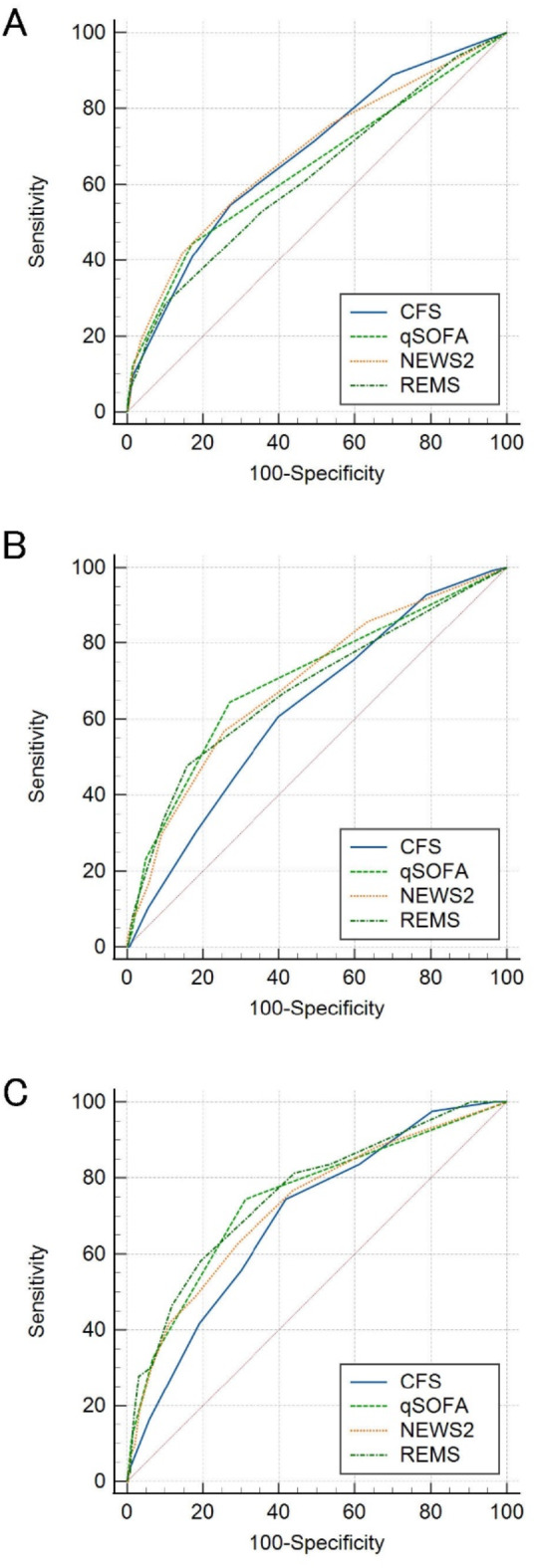
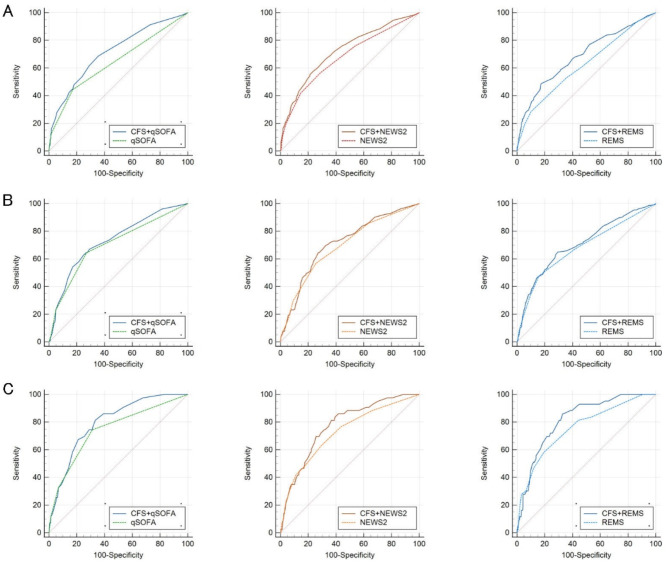
Vital signs are essential for monitoring and prognostication in the emergency department (ED); however, they may not fully capture the complexity of frailty in older adults. In this multicenter retrospective study of 932 older patients who visited the EDs of three tertiary university hospitals between August 1 and October 31, 2023, we investigated the prognostic value of the Clinical Frailty Scale (CFS) in older patients in the ED and its potential to improve existing vital sign-based scoring systems. The primary outcomes were hospital admission, intensive care unit (ICU) admission, and in-hospital mortality. The AUROC was used to evaluate and compare the predictive performance of CFS, qSOFA, NEWS2, and REMS scores individually and in combination. Combining the CFS with these scores significantly improved predictive accuracy compared to individual scores alone. For hospital admission, the AUROCs were 0.715 (95% CI 0.685-0.744), 0.723 (95% CI 0.693-0.752), and 0.688 (95% CI 0.657-0.718) for CFS + qSOFA, CFS + NEWS2, and CFS + REMS, respectively. For ICU admission, the AUROCs were 0.730 (95% CI 0.701-0.759), 0.714 (95% CI 0.684-0.743), and 0.707 (95% CI 0.677-0.736), respectively. For in-hospital mortality, the AUROCs were 0.798 (95% CI: 0.771-0.823), 0.774 (95% CI: 0.746-0.801), and 0.819 (95% CI: 0.793-0.843), respectively, indicating excellent performance. Incorporating frailty assessment using the CFS enhances risk stratification in older patients in the ED by complementing vital sign-based scores. This provides a more comprehensive assessment, enabling better informed clinical decisions. This study supports employing routine frailty assessment in the ED and the development of enhanced risk stratification tools that incorporate frailty.
Keywords: Clinical frailty scale (CFS); Emergency department (ED); Older people; Prognostic scoring systems; Risk stratification.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Prognostic value of frailty across age groups in emergency department patients aged 65 and above.BMC Geriatr. 2025 Jul 2;25(1):445. doi: 10.1186/s12877-025-06092-4. BMC Geriatr. 2025. PMID: 40604461 Free PMC article.
-
Comparison of early warning scores for predicting outcomes in adult and older patients in emergency department: Multicenter study.Am J Emerg Med. 2025 Jun 15;96:91-97. doi: 10.1016/j.ajem.2025.06.033. Online ahead of print. Am J Emerg Med. 2025. PMID: 40543431
-
Clinical Frailty Scale score is a predictor of short-, mid- and long-term mortality in critically ill older adults (≥ 70 years) admitted to the emergency department: an observational study.BMC Geriatr. 2024 Oct 21;24(1):852. doi: 10.1186/s12877-024-05463-7. BMC Geriatr. 2024. PMID: 39434029 Free PMC article.
-
Frailty assessment in emergency medicine using the Clinical Frailty Scale: a scoping review.Intern Emerg Med. 2022 Nov;17(8):2407-2418. doi: 10.1007/s11739-022-03042-5. Epub 2022 Jul 21. Intern Emerg Med. 2022. PMID: 35864373 Free PMC article.
-
Frailty-aware Care in the Emergency Department.Emerg Med Clin North Am. 2025 May;43(2):199-210. doi: 10.1016/j.emc.2024.08.004. Epub 2024 Sep 27. Emerg Med Clin North Am. 2025. PMID: 40210341 Review.
Cited by
-
Gaming Against Frailty: Effects of Virtual Reality-Based Training on Postural Control, Mobility, and Fear of Falling Among Frail Older Adults.J Clin Med. 2025 Aug 6;14(15):5531. doi: 10.3390/jcm14155531. J Clin Med. 2025. PMID: 40807152 Free PMC article.
-
The effectiveness of clinical frailty assessment in older patients with Traumatic brain injury in predicting outcome and quality of life: a systematic review.Neurosurg Rev. 2025 Jun 16;48(1):511. doi: 10.1007/s10143-025-03659-y. Neurosurg Rev. 2025. PMID: 40518500 Free PMC article. Review.
References
-
- Samaras, N., Chevalley, T., Samaras, D. & Gold, G. Older patients in the emergency department: A review. Ann. Emerg. Med.56, 261–269. 10.1016/j.annemergmed.2010.04.015 (2010). - PubMed
-
- Shenvi, C. L. & Platts-Mills, T. F. J. A. O. E. M. Managing the elderly emergency department patient. 73, 302–307 (2019). - PubMed
-
- Orsini, J. et al. Prognostic factors associated with adverse outcome among critically ill elderly patients admitted to the intensive care unit. 15, 889–894 (2015). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
