

ADORA2B promotes proliferation and migration in head and neck squamous cell carcinoma and is associated with immune infiltration
- PMID: 40221657
- PMCID: PMC11992813
- DOI: 10.1186/s12885-025-14102-2
ADORA2B promotes proliferation and migration in head and neck squamous cell carcinoma and is associated with immune infiltration
Abstract
Background: Adenosine A2B receptor (ADORA2B), a G protein-coupled receptor, is implicated in tumor progression and immune regulation in various cancers. However, its specific role in head and neck squamous cell carcinoma (HNSC) remains largely unexplored. This study aims to elucidate the expression profile, prognostic value, immune modulatory role, and therapeutic potential of ADORA2B in HNSC.
Methods: Comprehensive bioinformatics analyses were performed using TCGA and GEO datasets to evaluate ADORA2B expression, clinical correlations, and prognostic significance in HNSC. Weighted gene co-expression network analysis (WGCNA) and functional enrichment analyses were conducted to explore ADORA2B-associated pathways. Immune infiltration was assessed via ESTIMATE and single-sample gene set enrichment analysis (ssGSEA). Immune checkpoint blockade (ICB) therapy sensitivity and drug sensitivity were analyzed using the IMvigor210 and NCI-60 databases, respectively. In vitro experiments, including siRNA-mediated ADORA2B knockdown, CCK-8 assays, colony formation, and wound healing assays, were performed to validate the oncogenic role of ADORA2B.
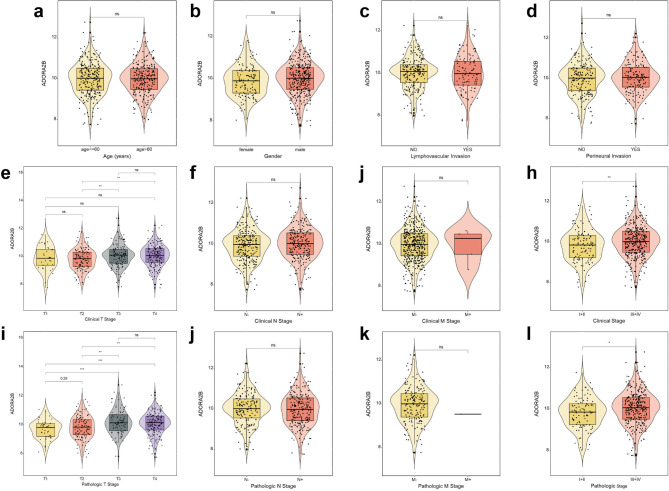
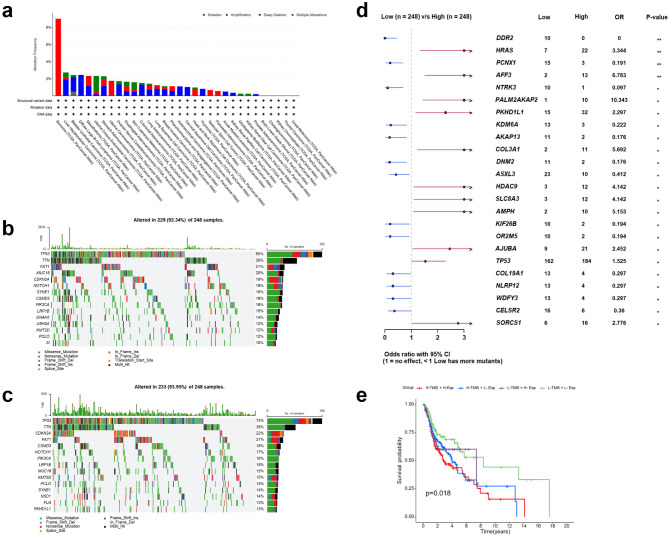
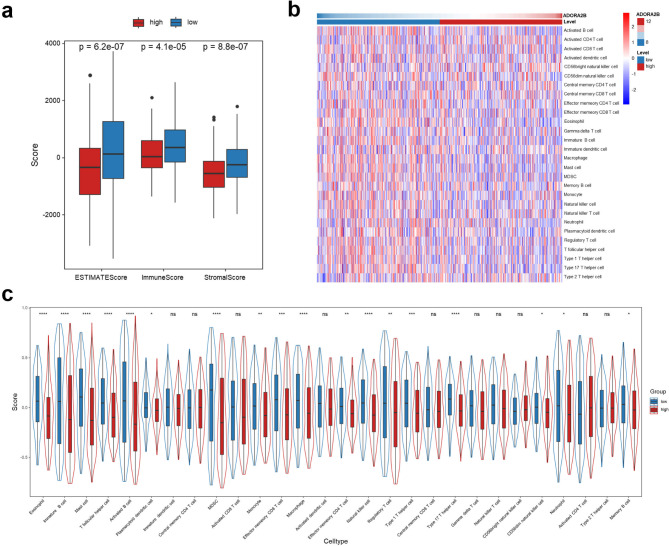
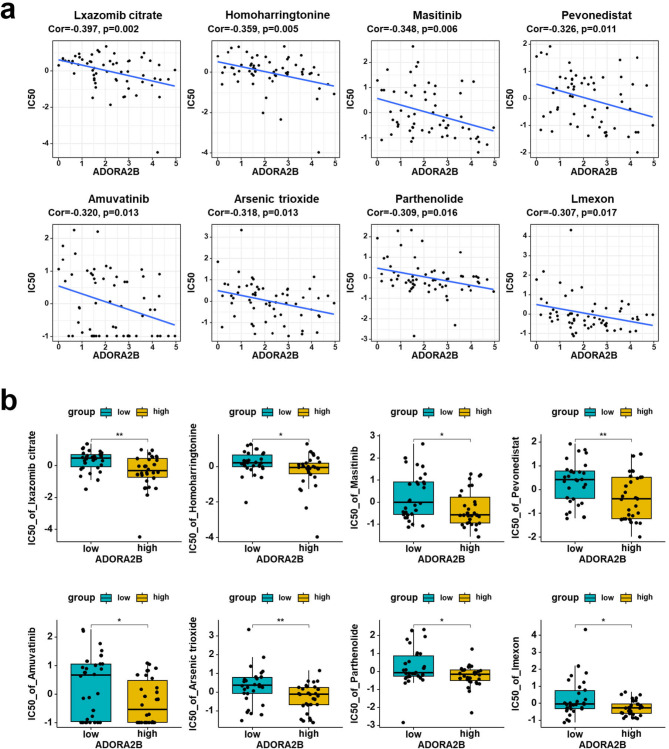
Results: ADORA2B was significantly overexpressed in HNSC tumor tissues compared to adjacent normal tissues, and its expression correlated with advanced clinical stage as well as poor overall survival (OS) and progression-free survival (PFS). Functional enrichment analyses revealed significant downregulation of immune-related pathways in high ADORA2B expression groups. High ADORA2B expression was associated with a more immunosuppressive tumor microenvironment (TME), characterized by lower immune and stromal scores and reduced immune cell infiltration. Immunotherapy response analysis demonstrated that patients with high ADORA2B expression exhibited poorer outcomes following ICB therapy. Drug sensitivity analysis identified several agents, including Ixazomib citrate, Masitinib, and others, as potential therapeutic candidates for high ADORA2B expression patients. In vitro experiments confirmed that ADORA2B knockdown significantly inhibited HNSC cell proliferation, colony formation, and migration, underscoring its critical role in tumor progression.
Conclusion: ADORA2B is a key oncogenic driver in HNSC, contributing to tumor proliferation, migration, and an immunosuppressive TME. Its high expression is associated with poor prognosis and reduced immunotherapy efficacy. Targeting ADORA2B may enhance therapeutic outcomes and overcome treatment resistance, highlighting its potential as a diagnostic, prognostic, and therapeutic biomarker.
Keywords: ADORA2B; Biomarker; HNSC; Immunotherapy; Tumor microenvironment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures







Similar articles
-
Identification of ETV4 as a prognostic biomarker and correlates with immune cell infiltration in head and neck squamous cell carcinoma.Sci Rep. 2025 Feb 27;15(1):7044. doi: 10.1038/s41598-025-90731-8. Sci Rep. 2025. PMID: 40016264 Free PMC article.
-
Comprehensive bioinformatics analysis of EXOSC family genes in head and neck squamous cell carcinoma.Sci Rep. 2025 Aug 19;15(1):30361. doi: 10.1038/s41598-025-15758-3. Sci Rep. 2025. PMID: 40830179 Free PMC article.
-
C16orf74 is a novel prognostic biomarker and associates with immune infiltration in head and neck squamous cell carcinoma.PLoS One. 2025 May 7;20(5):e0322701. doi: 10.1371/journal.pone.0322701. eCollection 2025. PLoS One. 2025. PMID: 40333816 Free PMC article.
-
Prognostic significance of Dickkopf-1 in head and neck squamous cell carcinoma.Expert Rev Anticancer Ther. 2024 Mar-Apr;24(3-4):147-154. doi: 10.1080/14737140.2023.2289597. Epub 2023 Dec 5. Expert Rev Anticancer Ther. 2024. PMID: 38044867 Review.
-
Intra-tumoral bacteria in head and neck cancer: holistic integrative insight.Cancer Biol Med. 2025 Feb 19;22(2):113-36. doi: 10.20892/j.issn.2095-3941.2024.0311. Cancer Biol Med. 2025. PMID: 39969204 Free PMC article. Review.
References
-
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. - PubMed
-
- Plath M, Gass J, Hlevnjak M, Li Q, Feng B, Hostench XP, et al. Unraveling most abundant mutational signatures in head and neck cancer. Int J Cancer. 2021;148(1):115–27. - PubMed
-
- Bhatia A, Burtness B. Treating head and neck cancer in the age of immunotherapy: A 2023 update. Drugs. 2023;83(3):217–48. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
