

Predictive model for initial response to first-line treatment in children with infantile epileptic spasms syndrome
- PMID: 40221729
- PMCID: PMC11993986
- DOI: 10.1186/s13052-025-01959-z
Predictive model for initial response to first-line treatment in children with infantile epileptic spasms syndrome
Abstract
Background: Previous studies have suggested that factors such as the treatment interval and aetiology may influence the initial response rate to first-line treatment for infantile epileptic spasms syndrome (IESS). However, few children with IECSS have undergone clinically accessible tests to determine the aetiology.
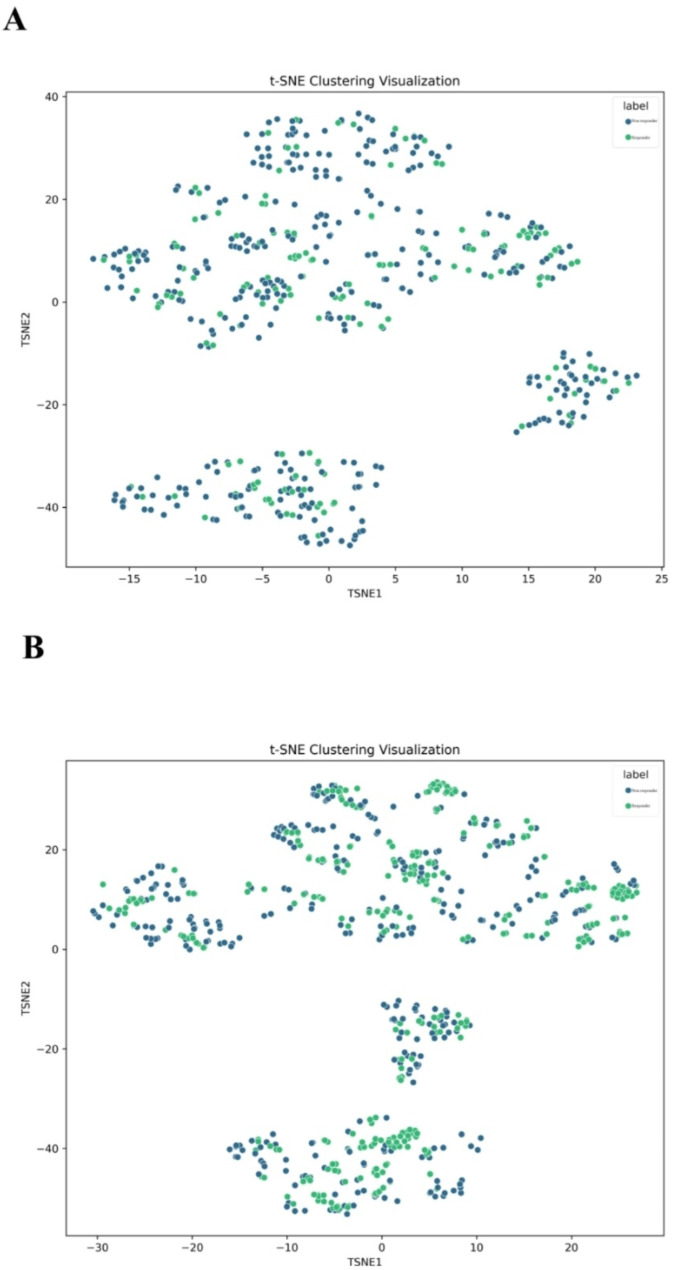
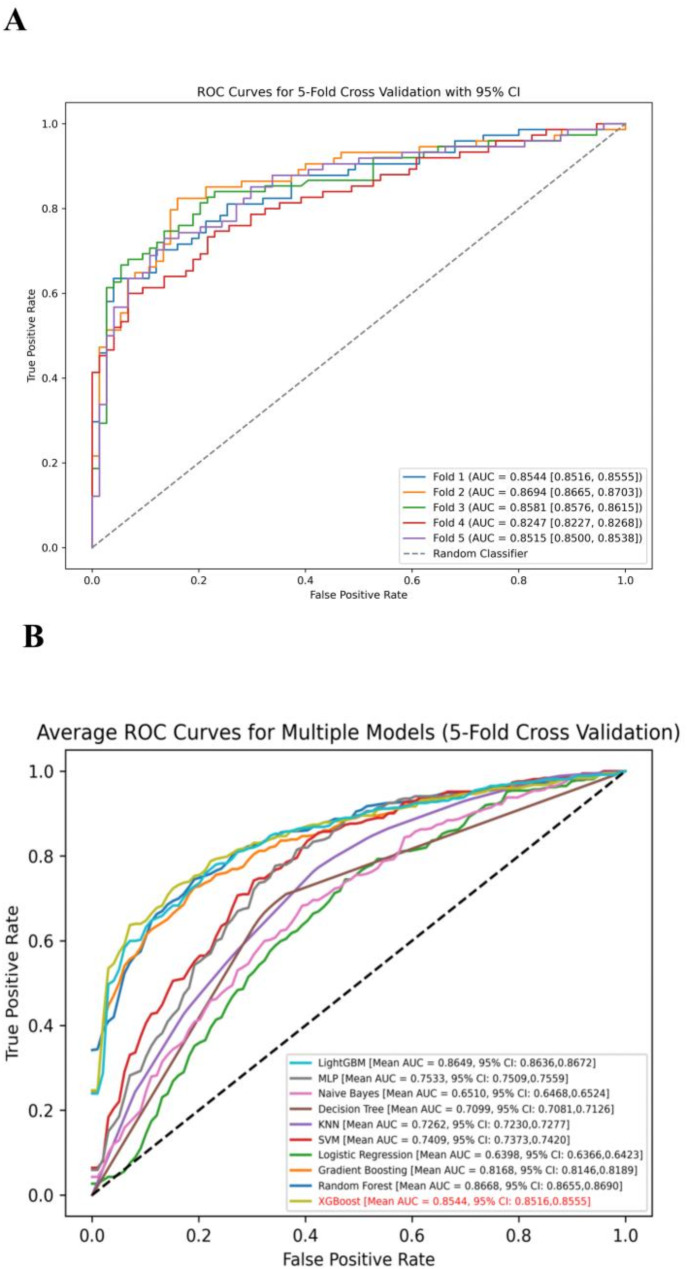
Methods: Using a dataset from our previously published research, we constructed and tested a predictive model for the initial response to first-line treatment in children with IESS. Random sampling and 5-fold cross-validation were performed, with synthetic minority oversampling technique to correct data imbalance. Machine learning algorithms and evaluation metrics optimised model accuracy and efficacy.
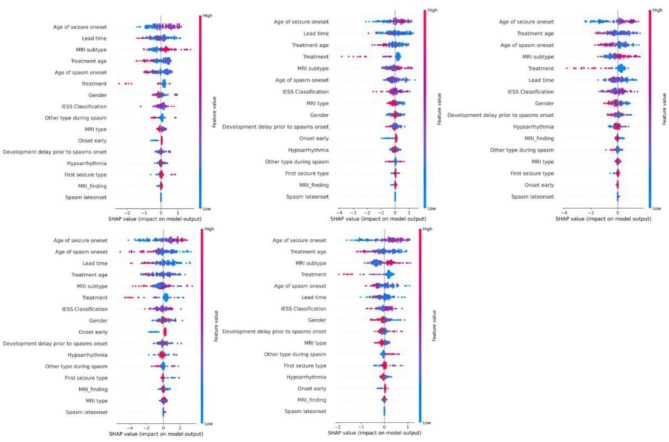
Results: This study included 532 children with IESS who had completed monotherapy first-line treatment, of whom 160 achieved an initial response. The model's accuracy, F1 score, and area under the curve (AUC) in the validation set were 0.7836 ± 0.0229 (ranging from 0.75167 to 0.80536), 0.7833 ± 0.0229 (ranging from 0.75145 to 0.80531), and 0.8516 ± 0.0165 (ranging from 0.82468 to 0.86936), respectively. Factors such as the age of seizure onset, age of spasm onset, lead time, MRI subtype, treatment choice, and age at treatment consistently ranked in the top six for importance in contributing to the model.
Conclusions: The study findings suggest that this model may help effectively predict the initial response to first-line treatment, supporting clinical decision-making for children with IESS. Key predictors such as the age of seizure onset and MRI subtype enable early, data-driven intervention strategies in clinical practice.
Keywords: First-line treatment; Infantile epileptic spasms syndrome (IESS); Initial response; Predictive model.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: Informed consent for participation in this study was obtained from the patient’s parents. Data are deidentified and protected by privacy safeguards. Ethical approval for the study was granted by the Ethics Committee of the First Medical Centre of the PLA General Hospital (S2020-337-01). Consent for publication: Written informed consent was obtained from the parents of the enrolled children. Competing interests: No financial or nonfinancial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures
Similar articles
-
Evaluating the effectiveness of medical therapy in infantile epileptic spasms syndrome due to surgically-remediable lesions.Epilepsia. 2025 May;66(5):1433-1446. doi: 10.1111/epi.18291. Epub 2025 Feb 13. Epilepsia. 2025. PMID: 39945474
-
Infantile epileptic spasms syndrome: When spasms come out of the blue.Epilepsy Behav. 2025 Feb;163:110180. doi: 10.1016/j.yebeh.2024.110180. Epub 2024 Dec 11. Epilepsy Behav. 2025. PMID: 39662322
-
Epileptic spasms relapse is associated with response latency but not conventional attributes of post-treatment EEG.Epilepsia Open. 2024 Jun;9(3):1034-1041. doi: 10.1002/epi4.12931. Epub 2024 Apr 8. Epilepsia Open. 2024. PMID: 38588009 Free PMC article.
-
Treatment modalities for infantile spasms: current considerations and evolving strategies in clinical practice.Neurol Sci. 2024 Feb;45(2):507-514. doi: 10.1007/s10072-023-07078-z. Epub 2023 Sep 22. Neurol Sci. 2024. PMID: 37736852 Review.
-
Infantile Spasms-Have We Made Progress?Curr Neurol Neurosci Rep. 2018 Apr 19;18(5):27. doi: 10.1007/s11910-018-0832-8. Curr Neurol Neurosci Rep. 2018. PMID: 29671077 Review.
References
-
- Riikonen R. Infantile spasms: outcome in clinical studies. Pediatr Neurol. 2020;108:54–64. 10.1016/j.pediatrneurol.2020.01.015 - PubMed
-
- Rajaraman RR, Smith RJ, Oana S, Daida A, Shrey DW, Nariai H, et al. Computational EEG attributes predict response to therapy for epileptic spasms. Clin Neurophysiol. 2024;163:39–46. 10.1016/j.clinph.2024.03.035 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
