

Arthroscopic-assisted uni-portal non-coaxial endoscopic surgery treatment of fibrous dysplasia of the femur: a minimally invasive alternative to open surgery
- PMID: 40221733
- PMCID: PMC11992799
- DOI: 10.1186/s12891-025-08617-9
Arthroscopic-assisted uni-portal non-coaxial endoscopic surgery treatment of fibrous dysplasia of the femur: a minimally invasive alternative to open surgery
Abstract
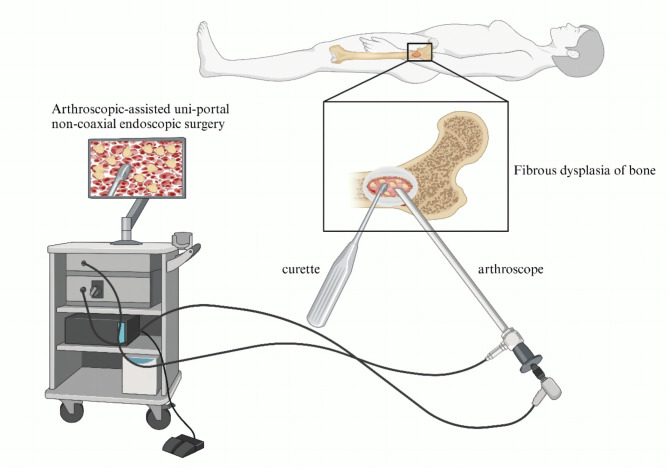
Background: Fibrous dysplasia of bone (FD) is a rare skeletal disorder. Traditional surgical options may have disadvantages such as greater trauma, incomplete curettage and recurrence risk. In this report, we introduce the technique for the treatment of fibrous dysplasia of the femur with Arthroscopic-assisted uni-portal non-coaxial endoscopic surgery (AUNES) and evaluate its feasibility.
Case presentation: We described a 49-year-old female patient with an elliptical lesion measuring approximately 4.3 cm × 4.2 cm in the proximal left femur. Due to the limitations of traditional open surgery-significant trauma, incomplete curettage, and a high risk of recurrence-we performed tumor curettage and bone graft fusion with AUNES assistance for the first time. The AUNES endoscopy provided a clear surgical field, precise lesion boundaries, thorough curettage, and minimal blood loss. Postoperative pathology confirmed fibrous dysplasia. At the 1-month and 3-month postoperative follow-ups, the patient's surgical wound healed well without complications. DR and CT scans showed satisfactory graft placement and bone fusion.
Conclusion: This case report demonstrates that AUNES-assisted tumor lesion curettage and bone grafting fusion surgery for FD is safe and feasible. It offers several advantages, including minimal invasiveness, a wide surgical field, thorough lesion curettage, and a low postoperative recurrence rate.
Keywords: Arthroscopic-assisted uni-portal non-coaxial endoscopic surgery; Fibrous dysplasia of bone; Minimally invasive.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics statement and consent to participate: All procedures performed in the study were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The review and reporting of the cases was in accordance with the ethical standards of the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University (Approval number: 2025-E0025). Consent for publication: Written informed consent was obtained from the patient for publication of this case report. Competing interests: The authors declare no competing interests.
Figures





References
-
- Russell LW, Chandler FA. Fibrous dysplasia of bone. J Bone Joint Surg Am. 1950;32A(2):321–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
