

Decreased CO2 saturation during circular breathwork supports emergence of altered states of consciousness
- PMID: 40223145
- PMCID: PMC11994804
- DOI: 10.1038/s44271-025-00247-0
Decreased CO2 saturation during circular breathwork supports emergence of altered states of consciousness
Abstract
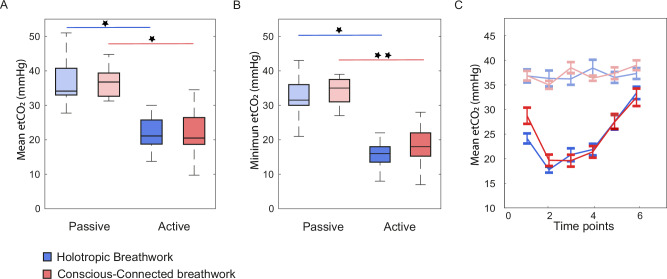
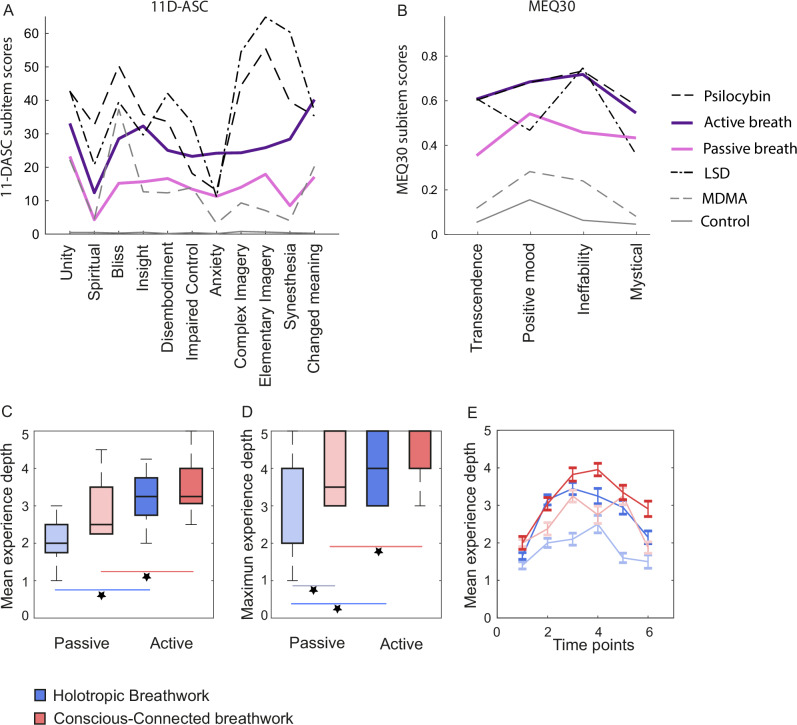
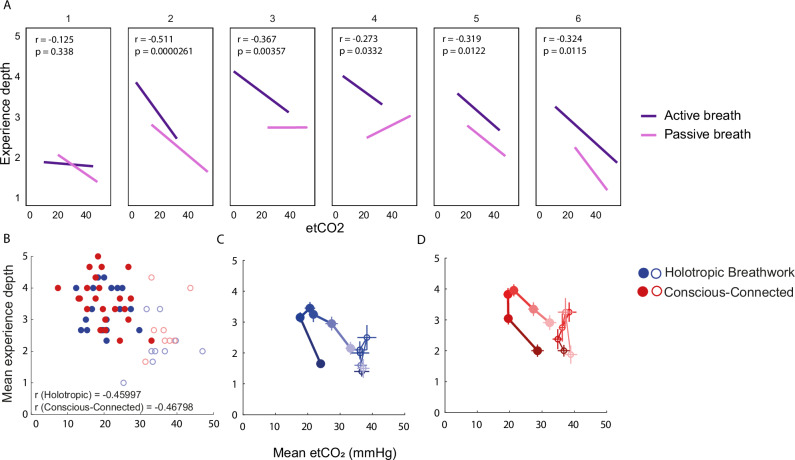
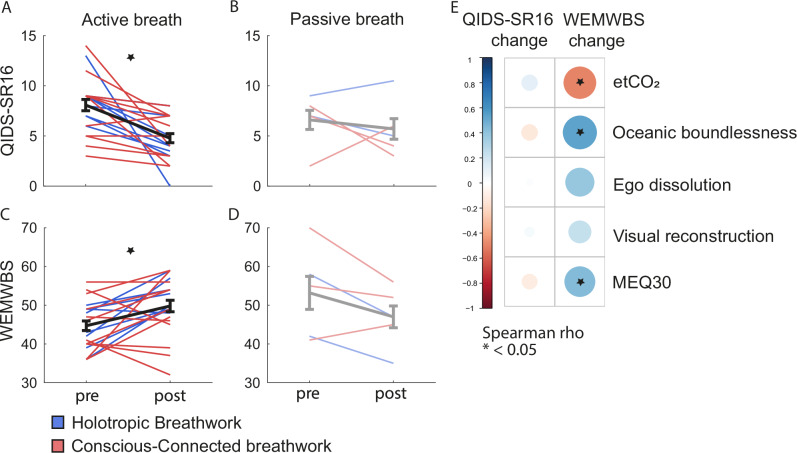
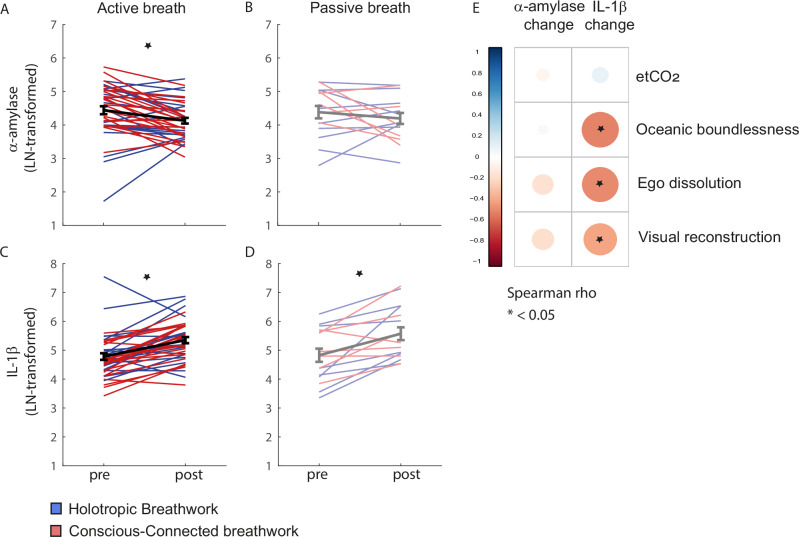
Altered states of consciousness (ASCs), induced e.g. during psychedelic-assisted therapy, show potential to treat prevalent mental health disorders like depression and posttraumatic stress disorder. However, access to such treatments is restricted by legal, medical, and financial barriers. Circular breathwork may present a non-pharmacological and hence more accessible alternative to engage similar therapeutic processes. Scientific studies of breathwork are only just emerging and its physiological and psychological mechanisms are largely unknown. Here, we track physiological and experiential dynamics throughout a breathwork session, comparing two forms of breathwork: Holotropic and Conscious-Connected breathwork. We show that a reduction in end-tidal CO2 pressure due to deliberate hyperventilation is significantly correlated to ASC onset (r = -0.46; p < 0.001). Based on standard questionnaires (MEQ-30 and 11-DASC), the ASCs evoked by breathwork resembled those produced by psychedelics across several experiential domains such as ego dissolution, and their depth predicted psychological and physiological follow-on effects, including improved well-being and reduced depressive symptoms. Further analysis showed that different breathwork approaches produced highly similar outcomes. Our findings identify physiological boundary conditions for ASCs to arise in a non-pharmacological context, shedding light on the functional mechanisms of breathwork as well as its potential as a psychotherapeutic tool.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: M.H. and M.L. are trained as facilitators of Conscious-Connected breathwork, and S.R., M.B. and L.V.-M. are trained as facilitators in Holotropic breathwork All co-authors declare no further competing interests.
Figures
Similar articles
-
Breathwork-induced psychedelic experiences modulate neural dynamics.Cereb Cortex. 2024 Aug 1;34(8):bhae347. doi: 10.1093/cercor/bhae347. Cereb Cortex. 2024. PMID: 39191666
-
Breathwork Interventions for Adults with Clinically Diagnosed Anxiety Disorders: A Scoping Review.Brain Sci. 2023 Feb 2;13(2):256. doi: 10.3390/brainsci13020256. Brain Sci. 2023. PMID: 36831799 Free PMC article.
-
Effect of breathwork on stress and mental health: A meta-analysis of randomised-controlled trials.Sci Rep. 2023 Jan 9;13(1):432. doi: 10.1038/s41598-022-27247-y. Sci Rep. 2023. PMID: 36624160 Free PMC article.
-
Phenomenology, Structure, and Dynamic of Psychedelic States.Curr Top Behav Neurosci. 2018;36:221-256. doi: 10.1007/7854_2016_459. Curr Top Behav Neurosci. 2018. PMID: 28025814 Review.
-
Holotropic Breathwork: the potential role of a prolonged, voluntary hyperventilation procedure as an adjunct to psychotherapy.J Altern Complement Med. 2007 Sep;13(7):771-6. doi: 10.1089/acm.2006.6203. J Altern Complement Med. 2007. PMID: 17931070 Review.
References
-
- Goodwin, G. M. et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N. Engl. J. Med.387, 1637–1648 (2022). - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous