

Long-Term Survival, Burden of Disease, and Patient-Centered Outcomes in Maximally Treated Intracerebral Hemorrhage
- PMID: 40223467
- PMCID: PMC12172108
- DOI: 10.1002/acn3.70048
Long-Term Survival, Burden of Disease, and Patient-Centered Outcomes in Maximally Treated Intracerebral Hemorrhage
Abstract
Objective: Increasing evidence shows that patients with intracerebral hemorrhage (ICH) can achieve better-than-expected outcomes with aggressive therapy. However, real-world long-term data, patient-centered outcomes, and societal measures after maximal ICH treatment are lacking. This study aimed to analyze 5-year survival, utility-weighted functional outcomes, and burden of disease in maximally treated ICH patients, stratified by max-ICH Score.
Methods: This study investigated consecutive patients with spontaneous ICH included in the single-center Longitudinal Cohort Study on ICH Care (UKER-ICH, NCT03183167, 2006-2015). We included all patients without early care limitations, hereinafter referred to as maximally treated. We analyzed the stratification by max-ICH Score of cumulative 5-year survival using Kaplan-Meier estimates and COX regression modeling, disease burden using disability-adjusted life years (DALYs), and patient-centered outcome at 12 months using the Utility-Weighted modified Rankin Scale (UW-mRS).
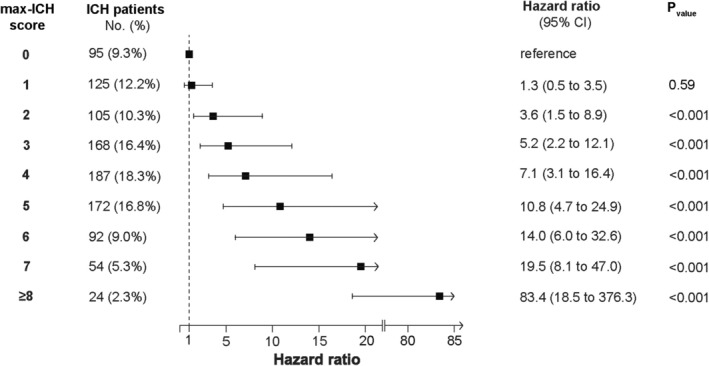
Results: The 5-year survival rate of the included 1022 maximally treated patients was 53%, stratified by max-ICH Score (0 points: 85%, 1: 91%, 2: 69%, 3: 59%, 4: 47%, 5: 32%, 6: 29%, 7: 18%, ≥ 8: 0%, log-rank p < 0.001). The mean number of DALYs was 8.94 (±8.15, standard deviation [SD]), consisting of 4.27 years of life lost (±7.79, SD) and 4.67 years lived with disability (±6.38, SD). Patients with a max-ICH Score of 5 had the highest burden of disease (12.76 [±9.43, SD]). The mean UW-mRS at 12 months was 0.45 (±0.37, SD) and decreased with increasing max-ICH Score (0: 0.80 [±0.23], 1: 0.73 [±0.29], 2: 0.67 [±0.29], 3: 0.50 [±0.34], 4: 0.39 [±0.34], 5: 0.25 [±0.30], 6: 0.19 [±0.28], 7: 0.16 [±0.26], ≥ 8: 0.08 [±0.22], p < 0.001).
Interpretation: These observational data, stratified by max-ICH Score, provide patients and treating physicians with an initial severity assessment in terms of potential long-term patient-centered outcomes and burden of disease following maximal treatment.
Keywords: intracerebral hemorrhage prognosis; patient‐centered outcomes; stroke disability burden.
© 2025 The Author(s). Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
M.I.S. reported receiving grants from the Interdisziplinäres Zentrum für Klinische Forschung, Marohn Foundation, Doktor Robert Pfleger‐Stiftung, and German Society for Neurointensive Care and Emergency Medicine (DGNI) for work outside the submitted work.
A.M. reports personal fees from Alexion Pharma Germany GmbH and Roche Pharma GmbH, outside the submitted work. J.A.S. reports personal fees from Lilly Deutschland GmbH, outside the submitted work.
Figures



References
-
- Greenberg S. M., Ziai W. C., Cordonnier C., et al., “2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association,” Stroke 53, no. 7 (2022): e282–e361. - PubMed
-
- Zahuranec D. B., Brown D. L., Lisabeth L. D., et al., “Early Care Limitations Independently Predict Mortality After Intracerebral Hemorrhage,” Neurology 68, no. 20 (2007): 1651–1657. - PubMed
-
- Becker K. J., Baxter A. B., Cohen W. A., et al., “Withdrawal of Support in Intracerebral Hemorrhage May Lead to Self‐Fulfilling Prophecies,” Neurology 56, no. 6 (2001): 766–772. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources