

Occurrence, Risk Factors, and Prognosis of Acute Cerebral Microinfarcts in CADASIL
- PMID: 40223500
- PMCID: PMC12172130
- DOI: 10.1002/acn3.70054
Occurrence, Risk Factors, and Prognosis of Acute Cerebral Microinfarcts in CADASIL
Abstract
Introduction: Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is the most common monogenic cerebral small vessel disease in adults. This study investigates the occurrence, risk factors, and prognosis of acute cerebral microinfarcts (ACMIs) in patients with CADASIL.
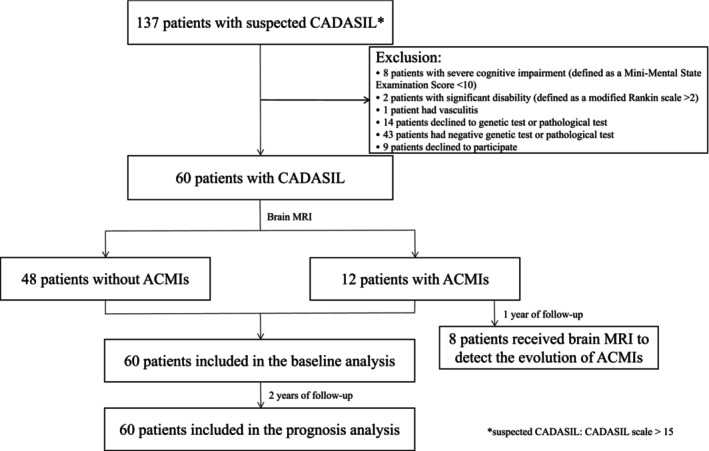
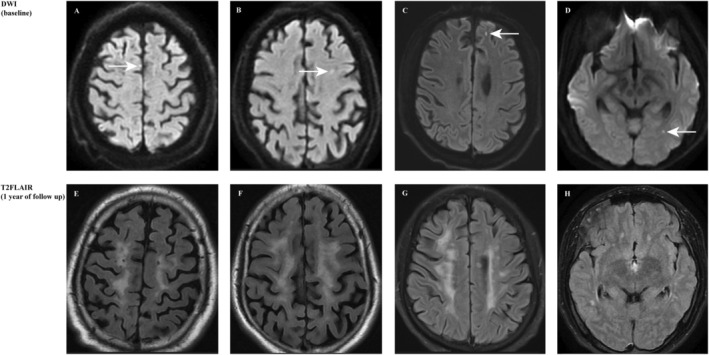
Methods: A total of 60 patients with genetically confirmed or pathologically verified CADASIL were enrolled in the study. ACMIs were identified as hyperintense lesions on diffusion-weighted imaging (DWI) with a diameter of less than 5 mm. The evolution of ACMIs was determined by brain MRI scans at 1 year of follow-up. Functional outcomes, cognitive performance, and quality of life after ACMIs were evaluated at months 6, 12, and 24, respectively.
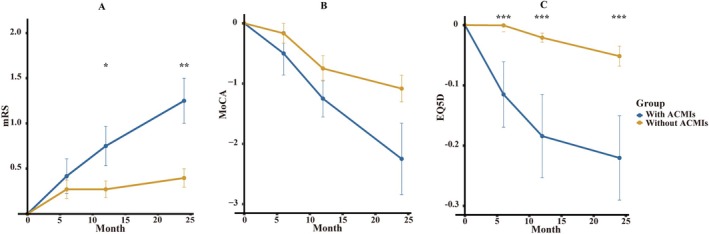
Results: ACMIs were observed in 12 out of 60 patients (20%) with CADASIL and predominantly located in the white matter. Patients with CADASIL had a significantly higher risk of ACMIs when they had a patent foramen ovale (PFO) (OR, 16.429). On follow-up MRI scans at month 12, the majority of ACMIs vanished. Patients with ACMIs had worse functional outcomes, as indicated by higher mRS scores and lower MoCA scores at months 12 and 24 compared with those without ACMIs. Additionally, patients with ACMIs had significantly worse EQ-5D-3L scores at all follow-up points compared with patients without ACMIs.
Conclusions: ACMIs were not rare in patients with CADASIL. PFO could independently predict the risk of ACMIs in CADASIL. Furthermore, the majority of ACMIs can disappear at 1 year of follow-up. The findings indicate that ACMIs, influenced by PFO, are prevalent in CADASIL and associated with a decline in quality of life and functional outcomes over time.
Keywords: CADASIL; PFO; acute cerebral microinfarcts.
© 2025 The Author(s). Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Guey S., Lesnik Oberstein S. A. J., Tournier‐Lasserve E., and Chabriat H., “Hereditary Cerebral Small Vessel Diseases and Stroke: A Guide for Diagnosis and Management,” Stroke 52 (2021): 3025–3032. - PubMed
-
- Ghosh M., Balbi M., Hellal F., Dichgans M., Lindauer U., and Plesnila N., “Pericytes Are Involved in the Pathogenesis of Cerebral Autosomal Dominant Arteriopathy With Subcortical Infarcts and Leukoencephalopathy,” Annals of Neurology 78 (2015): 887–900. - PubMed
-
- Opherk C., Peters N., Herzog J., Luedtke R., and Dichgans M., “Long‐Term Prognosis and Causes of Death in Cadasil: A Retrospective Study in 411 Patients,” Brain 127 (2004): 2533–2539. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources