

Gross anatomy, computed tomographic contrast tenography, and needle endoscopy of the equine medial digital flexor tendon sheath
- PMID: 40223504
- PMCID: PMC12344221
- DOI: 10.1111/vsu.14263
Gross anatomy, computed tomographic contrast tenography, and needle endoscopy of the equine medial digital flexor tendon sheath
Abstract
Objective: To investigate the computed tomography (CT) and gross anatomy of the equine medial digital flexor tendon sheath (MDFTS), and the endoscopic anatomy and approach to the MDFTS.
Study design: Ex vivo experimental study and one clinical case.
Sample population: Twelve clinically normal cadaveric hindlimbs.
Methods: Dissection, native and contrast CT scans were conducted to evaluate the anatomy of the MDFTS. Based on these findings, the portal locations for the endoscopic approaches were determined. Six hindlimbs were used in the pilot phase and another six limbs were selected for the main study. Endoscopic images were reviewed by three observers for the quality of visualization of intrasynovial structures during endoscopy.
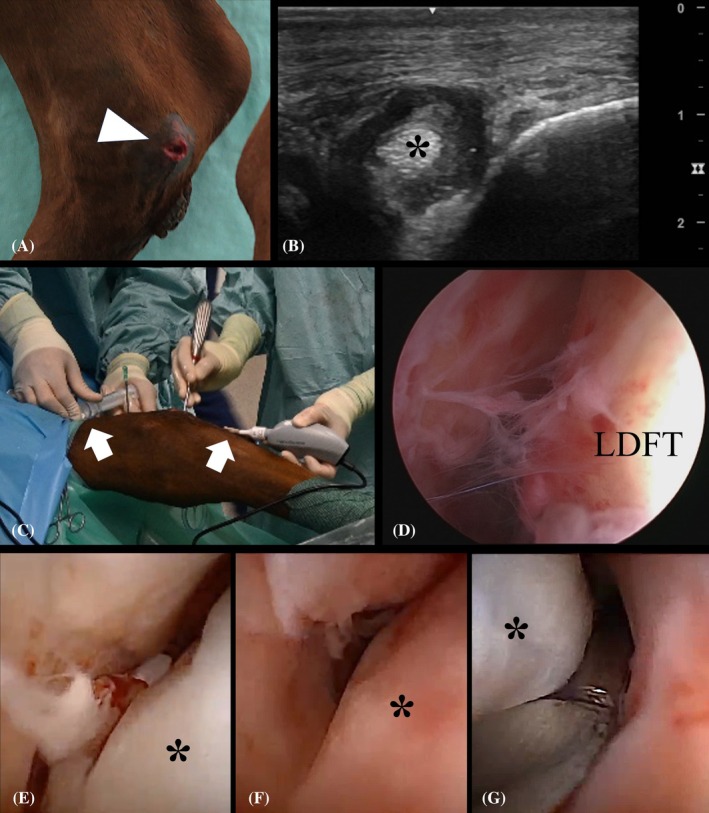
Results: Intrasynovial structures that could consistently be identified during dissection and CT examination included the mesotenon in the proximal recess and two synovial plicae surrounding the medial digital flexor tendon. Communication between MDFTS and tarsal sheath varied among individual horses. Two portals were necessary to visualize the complete length of the MDFTS. Endoscopic entry was possible with both a needle scope and a conventional arthroscope; however, endoscopic examination was only feasible with the needle scope. The aforementioned intrasynovial structures could also be visualized endoscopically. One clinical case is presented with septic tenosynovitis due to a laceration with penetration of the MDFTS.
Conclusion: Endoscopic examination of the MDFTS is possible with the use of a needle scope.
Clinical significance: Endoscopic lavage of the MDFTS might be indicated in cases of septic tenosynovitis of the MDFTS and/or tarsal sheath.
© 2025 The Author(s). Veterinary Surgery published by Wiley Periodicals LLC on behalf of American College of Veterinary Surgeons.
Conflict of interest statement
No conflict of interest to declare.
Figures



Similar articles
-
Equine non-septic tenosynovitis: A systematic literature review of site-specific pathological lesions, outcomes and surgical complications.Equine Vet J. 2024 Sep;56(5):842-857. doi: 10.1111/evj.14000. Epub 2023 Sep 21. Equine Vet J. 2024. PMID: 37735927
-
Efficacy of needle and endoscopic lavage on the recuperation of microspheres from the adult equine metacarpo-/metatarsophalangeal joint and digital flexor tendon sheath.Vet Surg. 2025 Aug;54(6):1157-1166. doi: 10.1111/vsu.14298. Epub 2025 Jun 25. Vet Surg. 2025. PMID: 40556484 Free PMC article.
-
Computed tomographic contrast tenography of the digital flexor tendon sheath of the equine hindlimb.Vet Radiol Ultrasound. 2018 May;59(3):279-288. doi: 10.1111/vru.12586. Epub 2017 Dec 22. Vet Radiol Ultrasound. 2018. PMID: 29274126
-
Elbow Fractures Overview.2025 Jul 7. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 7. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28723005 Free Books & Documents.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
References
-
- World Association of Veterinary Anatomists . International Committee on Veterinary Gross Anatomical Nomenclature. Nomina Anatomica Veterinaria. 6th ed. Editorial Committee; 2017.
-
- Wissdorf H, Gerhards H, Huskamp B. Praxisorientierte Anatomie Des Pferdes. Verlag M.& H. Schaper; 1998:412‐428.
-
- Dyson SJ. The deep digital flexor tendon. Diagnosis and Management of Lameness in the Horse. 2nd ed. Elsevier Inc.; 2011:726‐733.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
