

Long-term outcomes of active surveillance for Grade Group 1 prostate cancer and the impact of the use of MRI on overtreatment
- PMID: 40223578
- PMCID: PMC12256722
- DOI: 10.1111/bju.16727
Long-term outcomes of active surveillance for Grade Group 1 prostate cancer and the impact of the use of MRI on overtreatment
Abstract
Objectives: To present the long-term outcomes of men with Grade Group (GG) 1 prostate cancer (PCa), included in the Prostate Cancer Research International Active Surveillance (PRIAS) study, and to assess the effect of the inclusion of magnetic resonance imaging (MRI) within the active surveillance (AS) protocol.
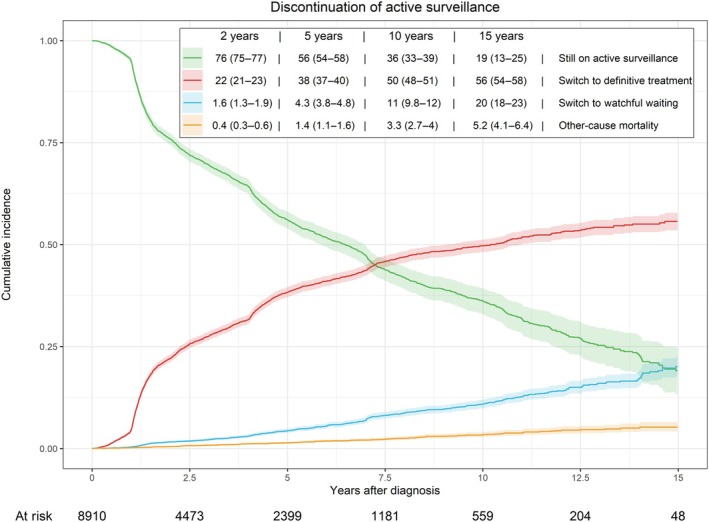
Patients and methods: The PRIAS study is a multicentre, prospective, web-based cohort study monitoring patients on AS. In total, 8910 men with GG1 PCa were followed in 169 centres worldwide. The cumulative incidences of definitive treatment, metastasis and PCa-specific mortality (PCSM) were estimated using competing risk analyses. Additionally, multivariable analysis was performed to assess the risk of reclassification, stratified by MRI performed around the time of diagnosis.
Results: The cumulative incidence of definitive treatment 15 years post-diagnosis was 55% (95% confidence interval [CI] 53-57). For metastasis, the 15-year cumulative incidence was 2.7% (95% CI 1.5-4.4). Eight men of died from PCa, resulting in a 15-year cumulative PCSM incidence of 0.23% (95% CI 0.09-0.54). Compared to men with no MRI around the time of diagnosis, those who underwent MRI during the first 18 months of AS were associated with a significantly higher risk of reclassification to ≥GG2, while men with a positive MRI before diagnosis were associated with a higher risk of reclassification to GG2, but not to ≥GG3. Men with GG2 PCa on MRI-targeted rebiopsy who underwent definitive treatment did not show a statistically significant higher risk of 5-year disease recurrence compared to those who had GG1 PCa on last biopsy during AS.
Conclusions: Our study confirms the safety of AS for GG1 PCa, with low metastasis and PCSM rates over 15 years. Furthermore, the inclusion of MRI in AS prompts increased detection of GG2, leading to increased treatment rates despite similar short-term risks. To minimise overtreatment, expanding eligibility for AS and the uptake of AS in men with favourable GG2 PCa is crucial to address the stage shift resulting from the increased accuracy of MRI.
Keywords: active surveillance; magnetic resonance imaging; metastatic disease; mortality; prostatic neoplasms.
© 2025 The Author(s). BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Figures

References
-
- van den Bergh RCN, Roemeling S, Roobol MJ, Roobol W, Schröder FH, Bangma CH. Prospective validation of active surveillance in prostate cancer: the PRIAS study. Eur Urol 2007; 52: 1560–1563 - PubMed
-
- Bokhorst LP, Valdagni R, Rannikko A et al. A decade of active surveillance in the PRIAS study: an update and evaluation of the criteria used to recommend a switch to active treatment. Eur Urol 2016; 70: 954–960 - PubMed
-
- Ashwin SB, Janet EC, Matthew RC, Katsuto S, Hao GN, Peter RC. Evaluating the safety of active surveillance: outcomes of deferred radical prostatectomy after an initial period of surveillance. J Urol 2019; 202: 506–510 - PubMed
-
- Tosoian JJ, Mamawala M, Epstein JI et al. Active surveillance of grade group 1 prostate cancer: long‐term outcomes from a large prospective cohort. Eur Urol 2020; 77: 675–682 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
