

A retrospective analysis of oral autoimmune bullous diseases at a Thai oral medicine center
- PMID: 40224110
- PMCID: PMC11993048
- DOI: 10.1016/j.jds.2024.10.002
A retrospective analysis of oral autoimmune bullous diseases at a Thai oral medicine center
Abstract
Background: /Purpose Autoimmune bullous diseases (AIBDs) are rare conditions that can affect daily life and be life-threatening. However, there is scant research on Thai patients with oral AIBDs.
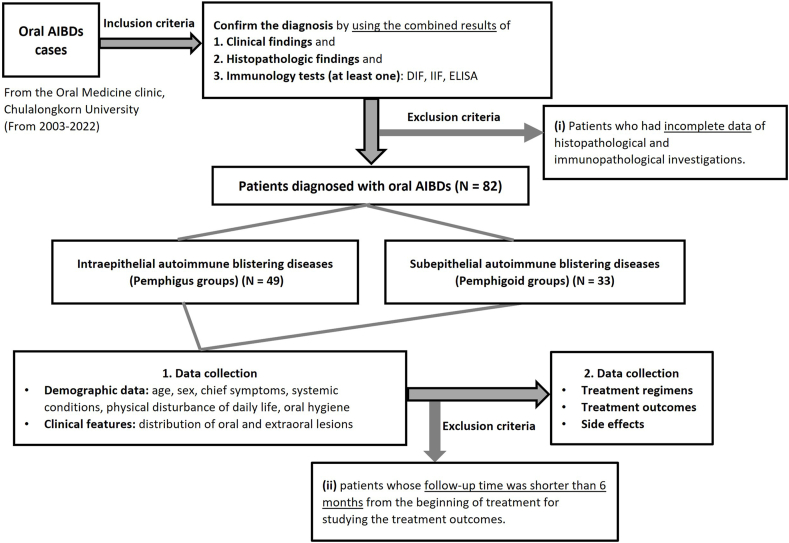
Materials and methods: Retrospective analysis of the characteristics, distribution, and treatment outcomes of oral AIBDs in Thai patients (20-year period).
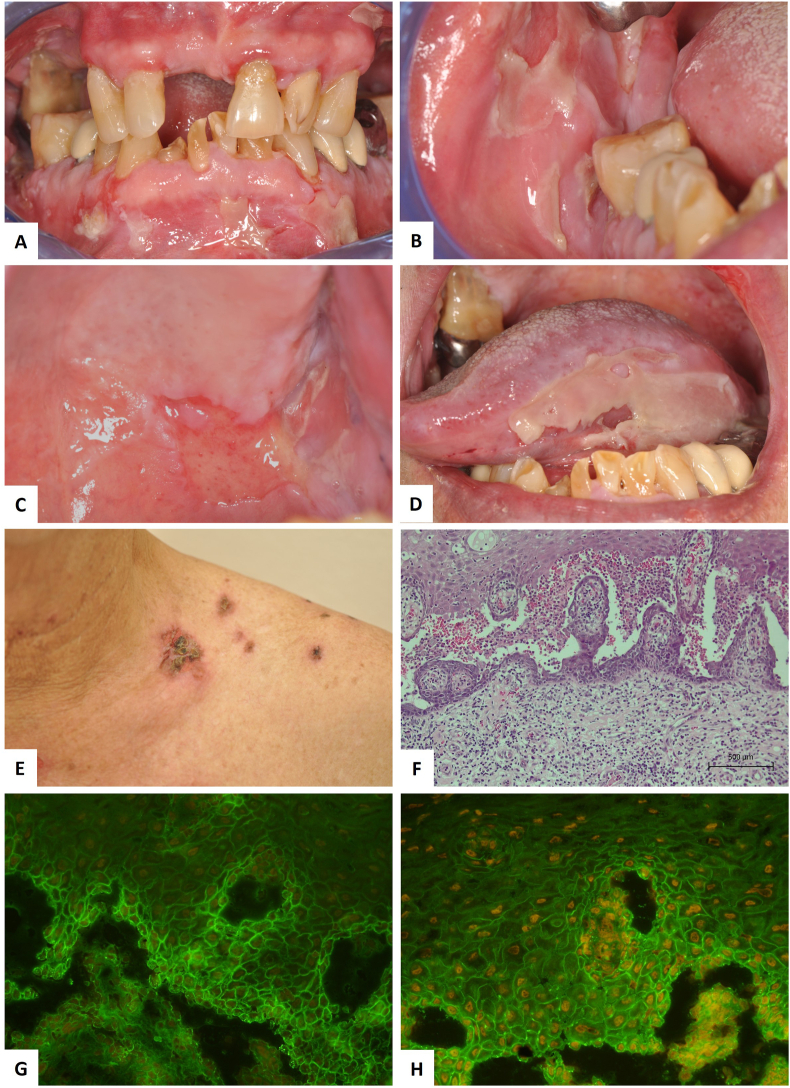
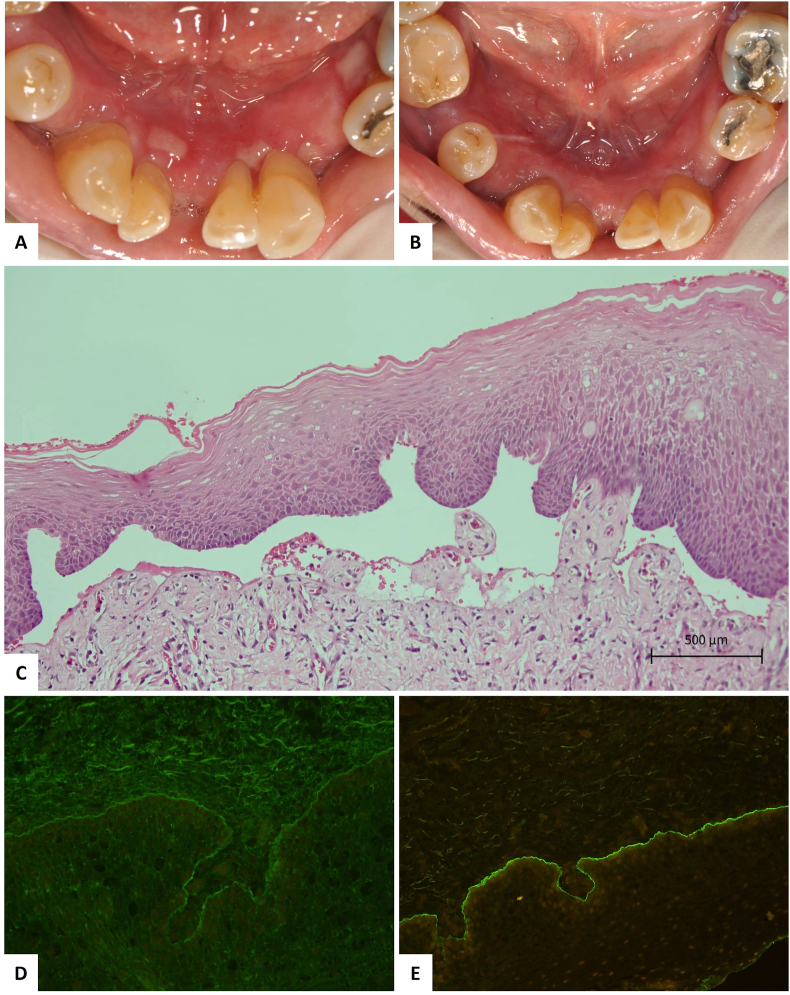
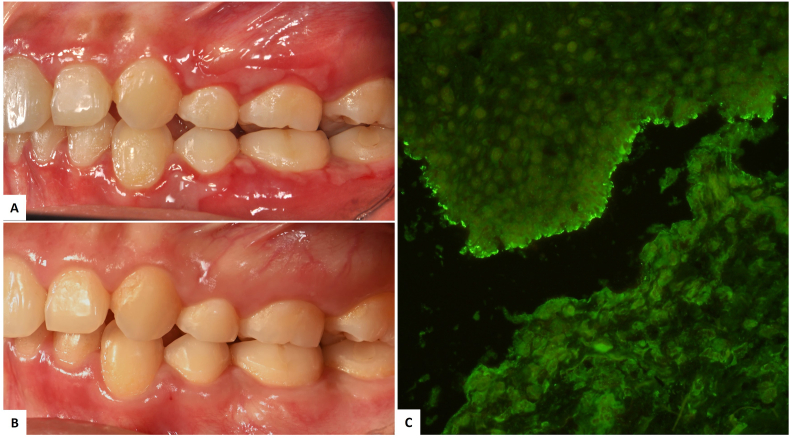
Results: Eighty-two oral AIBDs patients were diagnosed, mostly female ages ranging from middle-aged to elderly. The most common subtype was pemphigus vulgaris (PV) (59.8 %), followed by mucous membrane pemphigoid (MMP) (26.8 %), bullous pemphigoid (BP) (8.5 %), and linear IgA bullous dermatosis (LABD) (4.9 %). The gingiva was the most affected site. Notably, 81.8 % of MMP patients had only oral lesions (mostly gingiva), while most PV patients had multiple lesions, with oral lesions often appearing first. Corticosteroids (CS) (topical and/or systemic) were the primary treatment. The overall response rate for control of disease activity (CDA) was 73.9 %, with complete remission (CR) in 17.4 %. Patients receiving only topical CS had fewer side effects (66.7 % reported none, others mild) compared with combined therapy (48.6 % reported side effects).
Conclusion: PV was the most prevalent subtype, often presenting with oral and skin lesions, with oral lesions appearing first. Conversely, MMP primarily manifested as isolated oral lesions, often with desquamative gingivitis. Combination therapy with topical and systemic CS was the most common treatment for oral AIBDs. Notably, patients treated with topical CS only experienced significantly fewer and milder side effects compared with those receiving other treatments.
Keywords: Linear IgA bullous dermatosis; Mucous membrane pemphigoid; Oral autoimmune bullous diseases; Pemphigoid; Pemphigus vulgaris; Thai.
© 2025 Association for Dental Sciences of the Republic of China. Publishing services by Elsevier B.Vé.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article.
Figures
Similar articles
-
Retrospective analysis of autoimmune bullous diseases in Middle Franconia.Front Immunol. 2023 Oct 10;14:1256617. doi: 10.3389/fimmu.2023.1256617. eCollection 2023. Front Immunol. 2023. PMID: 37881435 Free PMC article.
-
Oral mucous membrane pemphigoid and pemphigus vulgaris-a retrospective two-center cohort study.Oral Dis. 2017 May;23(4):498-504. doi: 10.1111/odi.12639. Epub 2017 Feb 22. Oral Dis. 2017. PMID: 28084005
-
Rituximab Therapy for Mucous Membrane Pemphigoid: A Retrospective Monocentric Study With Long-Term Follow-Up in 109 Patients.Front Immunol. 2022 Jun 30;13:915205. doi: 10.3389/fimmu.2022.915205. eCollection 2022. Front Immunol. 2022. PMID: 35844526 Free PMC article.
-
Autoimmune mucocutaneous blistering diseases after SARS-Cov-2 vaccination: A Case report of Pemphigus Vulgaris and a literature review.Pathol Res Pract. 2022 Apr;232:153834. doi: 10.1016/j.prp.2022.153834. Epub 2022 Mar 5. Pathol Res Pract. 2022. PMID: 35278817 Free PMC article. Review.
-
Uncommon and Unusual Variants of Autoimmune Bullous Diseases.Indian Dermatol Online J. 2024 Aug 30;15(5):739-748. doi: 10.4103/idoj.idoj_755_23. eCollection 2024 Sep-Oct. Indian Dermatol Online J. 2024. PMID: 39359270 Free PMC article. Review.
References
-
- Sun S., Zhong B., Li W., et al. Immunological methods for the diagnosis of oral mucosal diseases. Br J Dermatol. 2019;181:23–36. - PubMed
-
- Montagnon C.M., Tolkachjov S.N., Murrell D.F., Camilleri M.J., Lehman J.S. Intraepithelial autoimmune blistering dermatoses: clinical features and diagnosis. J Am Acad Dermatol. 2021;84:1507–1519. - PubMed
-
- Kridin K. Pemphigus group: overview, epidemiology, mortality, and comorbidities. Immunol Res. 2018;66:255–270. - PubMed
-
- Daniel B.S., Murrell D.F. Review of autoimmune blistering diseases: the pemphigoid diseases. J Eur Acad Dermatol Venereol. 2019;33:1685–1694. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
