

A nomogram based on systemic inflammation response index and clinical risk factors for prediction of short-term prognosis of very elderly patients with hypertensive intracerebral hemorrhage
- PMID: 40224624
- PMCID: PMC11985803
- DOI: 10.3389/fmed.2025.1535443
A nomogram based on systemic inflammation response index and clinical risk factors for prediction of short-term prognosis of very elderly patients with hypertensive intracerebral hemorrhage
Abstract
Objective: To develop and validate a nomogram based on systemic inflammation response index (SIRI) and clinical risk factors to predict short-term prognosis in very elderly patients with hypertensive intracerebral hemorrhage (HICH).
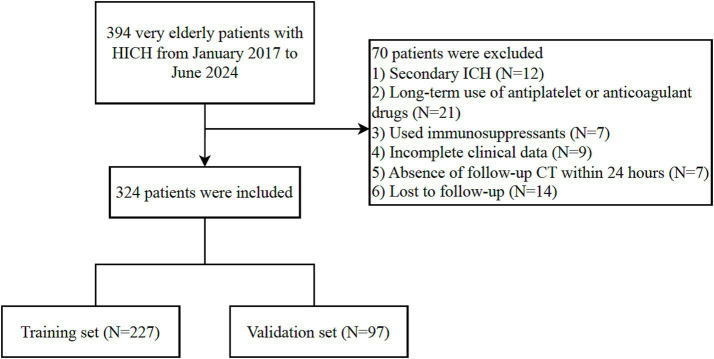
Methods: A total of 324 very elderly HICH patients from January 2017 to June 2024 were retrospectively enrolled and randomly divided into two cohorts for training (n = 227) and validation (n = 97) according to the ratio of 7:3. Independent predictors of poor prognosis were analyzed using univariate and multivariate logistic regression analyses. Furthermore, a nomogram prediction model was built. The area under the receiver operating characteristic curves (AUC), calibration plots and decision curve analysis (DCA) were used to evaluate the performance of the nomogram in predicting the prognosis of very elderly HICH.
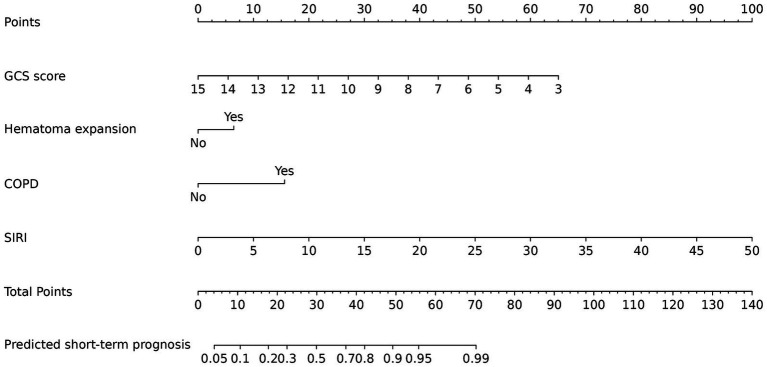
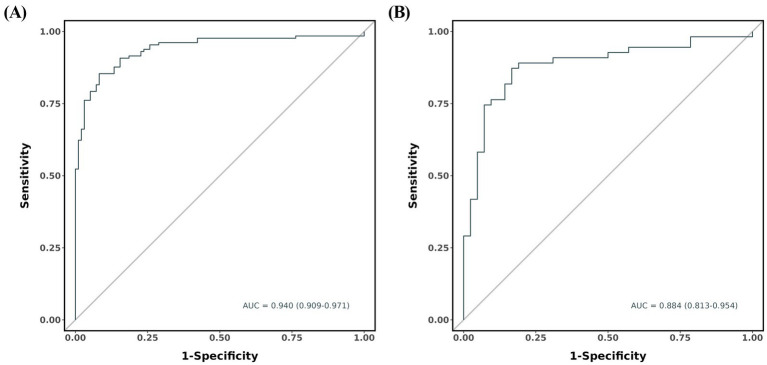
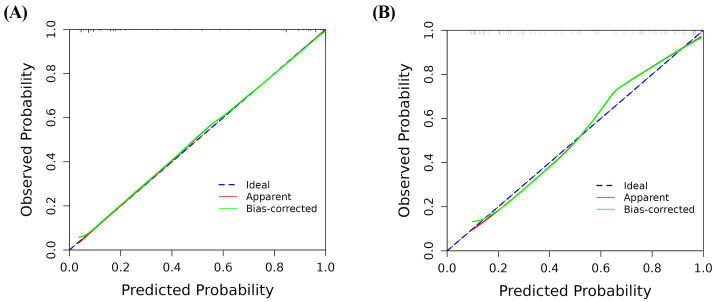
Results: By univariate and stepwise multivariate logistic regression analyses, GCS score (p < 0.001), hematoma expansion (p = 0.049), chronic obstructive pulmonary disease (p = 0.010), and SIRI (p = 0.005) were independent predictors for the prognosis in very elderly patients with HICH. The nomogram showed the highest predictive efficiency in the training cohort (AUC = 0.940, 95% CI: 0.909 to 0.971) and the validation cohort (AUC = 0.884, 95% CI: 0.813 to 0.954). The calibration curve indicated that the nomogram had good calibration. DCA showed that the nomogram had high applicability in clinical practice.
Conclusion: The nomogram incorporated with the SIRI and clinical risk factors has good potential in predicting the short-term prognosis of very elderly HICH.
Keywords: nomogram; poor prognosis; risk factors; systemic inflammation response index; very elderly hypertensive intracerebral hemorrhage.
Copyright © 2025 Wang, Wang, Li, Liu, Lai, Sun and Hu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
A Nomogram Based on CT Radiomics and Clinical Risk Factors for Prediction of Prognosis of Hypertensive Intracerebral Hemorrhage.Comput Intell Neurosci. 2022 Dec 7;2022:9751988. doi: 10.1155/2022/9751988. eCollection 2022. Comput Intell Neurosci. 2022. PMID: 36531926 Free PMC article.
-
Prediction of short-term prognosis of patients with hypertensive intracerebral hemorrhage by radiomic-clinical nomogram.Front Neurol. 2023 Feb 3;14:1053846. doi: 10.3389/fneur.2023.1053846. eCollection 2023. Front Neurol. 2023. PMID: 36816560 Free PMC article.
-
Prognostic value of nomogram model based on clinical risk factors and CT radiohistological features in hypertensive intracerebral hemorrhage.Front Neurol. 2024 Dec 4;15:1502133. doi: 10.3389/fneur.2024.1502133. eCollection 2024. Front Neurol. 2024. PMID: 39697438 Free PMC article.
-
Prediction of Hematoma Expansion in Hypertensive Intracerebral Hemorrhage by a Radiomics Nomogram.Pak J Med Sci. 2023 Jul-Aug;39(4):1149-1155. doi: 10.12669/pjms.39.4.7724. Pak J Med Sci. 2023. PMID: 37492285 Free PMC article.
-
Establishment and evaluation of a nomogram model for predicting hematoma expansion in hypertensive intracerebral hemorrhage based on clinical factors and plain CT scan signs.Ann Palliat Med. 2021 Dec;10(12):12789-12800. doi: 10.21037/apm-21-3569. Ann Palliat Med. 2021. PMID: 35016444
References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral Haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. (2010) 9:167–76. doi: 10.1016/s1474-4422(09)70340-0, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources