

Real-world use of complement inhibitors for haemolytic uraemic syndrome: an analysis of the European Rare Kidney Disease Registry cohort
- PMID: 40224677
- PMCID: PMC11987679
- DOI: 10.1016/j.eclinm.2025.103159
Real-world use of complement inhibitors for haemolytic uraemic syndrome: an analysis of the European Rare Kidney Disease Registry cohort
Abstract
Background: Although terminal complement inhibitors transformed the prognosis of atypical haemolytic uraemic syndrome (aHUS) from dismal to favourable, treatment approaches vary due to the intermittent disease nature and high costs. Occasionally, complement inhibition is applied in infectious (i)HUS. We aimed to examine real-world C5 inhibitor use and its impact on patient outcomes.
Methods: This retrospective cohort study used longitudinal data from the European Rare Kidney Disease Registry, collected from 76 nephrology centres across 24 European countries between January 1, 2019 and January 31, 2024. Eligible patients had aHUS or iHUS with onset after January 1, 2011, and/or documented C5 inhibitor use. Exclusions included complement-unrelated HUS, post-transplant HUS, and prophylactic C5 inhibitor use around kidney transplantation. Data, derived from medical records and focused queries, were used to assess C5 inhibitor duration, via time-to-event analysis, and kidney function based on annual creatinine levels.
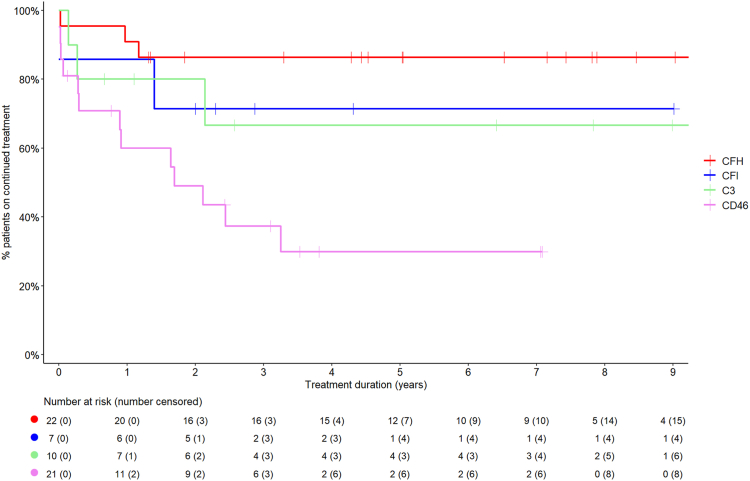
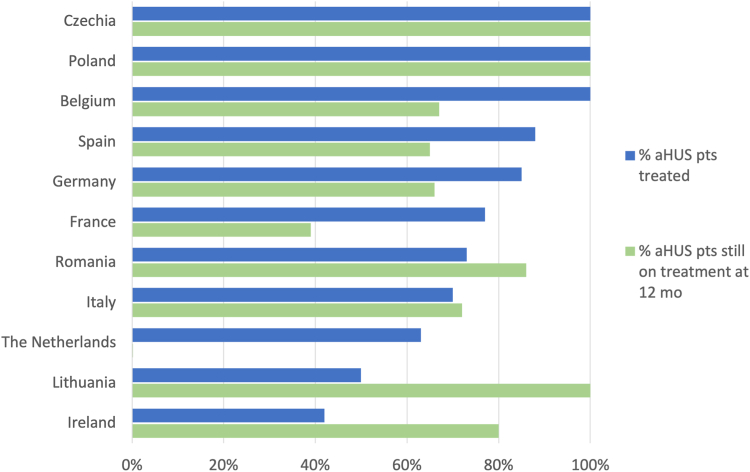
Findings: A total of 238 aHUS and 472 patients with iHUS were included in the analysis. C5 inhibition was applied in 76.5% of aHUS and 18.4% of iHUS, with major utilisation differences between countries (p < 0.0001) and less common use in female patients with aHUS (p = 0.0022). Median (interquartile range) treatment duration was 16.1 (3.6-41.2) months in aHUS and 9 (7-32) days in iHUS. After five years, 56% of genetic, 28% of anti-complement factor H (anti-CFH) antibody-mediated, and 23% of aHUS cases with no identified cause remained on treatment. The long-term (>7 years) risk of treatment resumption was 35% in genetic, 15% in aHUS of no identified cause, and 0% in anti-CFH antibody-mediated aHUS. Post-withdrawal aHUS relapses were mostly mild and did not lead to permanent kidney function impairment, ultimately leading to long-term treatment withdrawal in 92.5% of discontinued cases.
Interpretation: Currently, C5 inhibitors are administered in three-quarters of newly diagnosed patients with aHUS in Europe, with varied utilisation and discontinuation practices. Treatment withdrawal is common and safe, although relapses may occur, particularly in genetic aHUS. However, baseline disease severity, selective use in expert centres, and indication bias affect outcome comparability. Findings must be considered in the context of patient-specific factors and disease severity at the time of treatment decisions.
Funding: This research was supported by the European Reference Network for Rare Kidney Diseases, funded by the European Union within the framework of the "EU4Health Programme 2021-2027".
Keywords: Complement inhibitor; European Rare Kidney Disease Registry; Haemolytic uraemic syndrome; Post-withdrawal relapse; Treatment discontinuation.
© 2025 The Authors.
Conflict of interest statement
All authors declare the following potential conflicts of interest related to the content of this manuscript: MCM received speaker honoraria and a travel grant from Alexion. OB received speaker honoraria from Alexion and Samsung. AA served on the Data Monitoring Committee for the UK trial on C5 inhibitor discontinuation. MF received speaker honoraria, payment for expert testimony, consultancy fees, and a travel grant from Alexion. GA received speaker honoraria and travel grants from Alexion (AstraZeneca Rare Diseases) and served on its Board. JH works as a statistician at ERKNet, which received payments from Vertex, Novartis, and Sobi for research collaborations. JH performed statistical analyses and created project reports on behalf of ERKNet: “Analysis of the ERKReg database for ADPKD & AMKD studies” for Vertex, “Disease characteristics and treatment patterns of C3G and IC-MPGN in Europe: a multicentre retrospective analysis using the ERKReg database” for Novartis, and “A C3G and Primary IC-MPGN Retrospective Observational Study - Fit-For-Purpose Summary Report” for Sobi. MV received consultancy fees from Novartis, BioCryst, Roche, Apellis, speaker honoraria from Roche, Novartis, Alexion, Vifor, and Travere, and a grant from the Italian Ministry of Health to her institution. NCAJVDK received grants from Apellis and Novartis as principal or sub-investigator for international trials on pegcetacoplan and iptacopan for C3G treatment, consulting fees from Samsung, Alexion, and Novartis, speaker fees from Novartis and Sobi, travel grants from Samsung and Sobi, and served on a board for Roche, with all payments made to her institution. FS received consulting fees from Samsung Bioepis for participation in Scientific Advisory Board meetings, with payment made to him, and from Alexion for consulting on paediatric trial programs in potential new indications for C5 inhibitors while participating in the sAlexion Global aHUS Registry Steering Committee, with payments made to his institution. The remaining authors declare no conflicts of interest. No other relevant affiliations or financial involvements exist beyond those disclosed.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous
