

Thromboelastography Reference Values for Third-Trimester Healthy Obstetric Patients in Northern Mexico
- PMID: 40225040
- PMCID: PMC11991821
- DOI: 10.1155/anrp/8871619
Thromboelastography Reference Values for Third-Trimester Healthy Obstetric Patients in Northern Mexico
Abstract
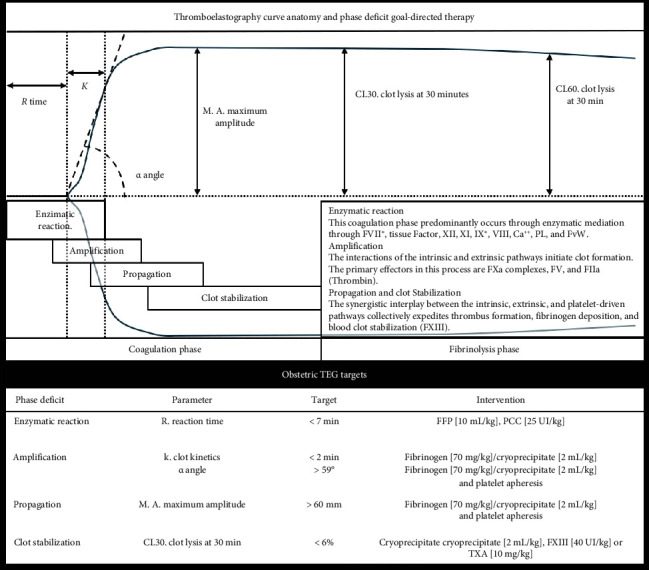
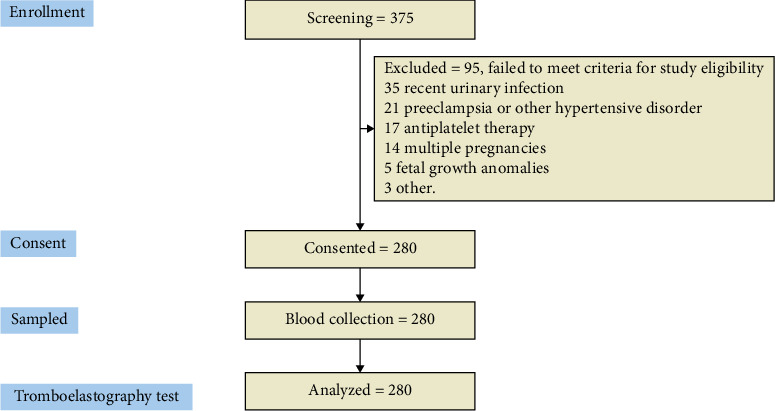
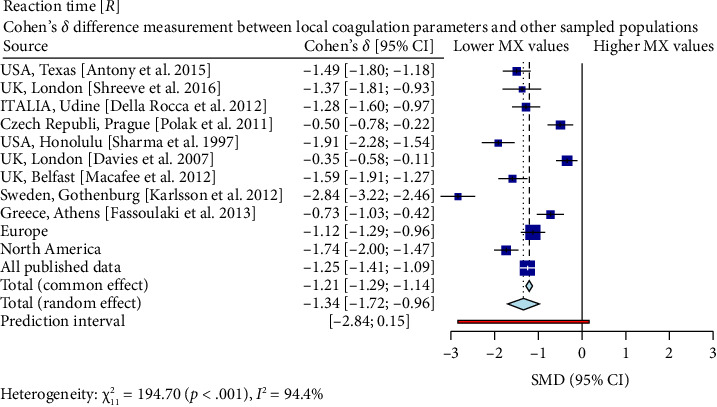
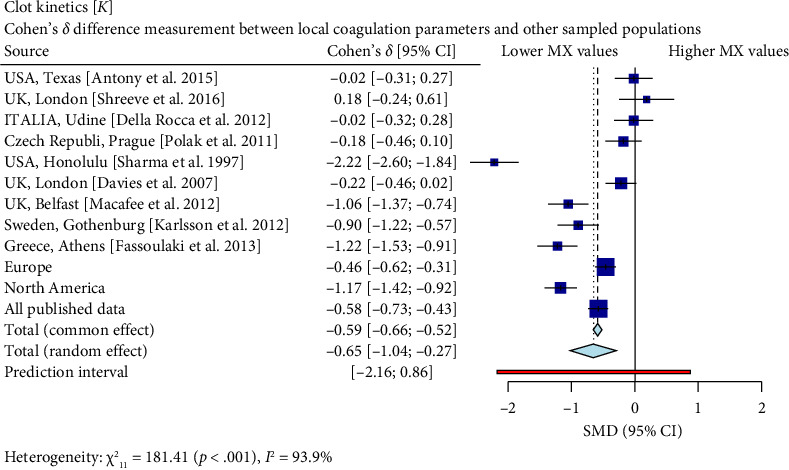
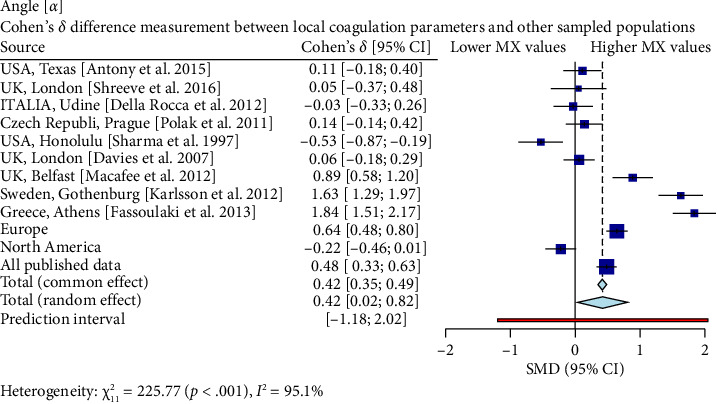
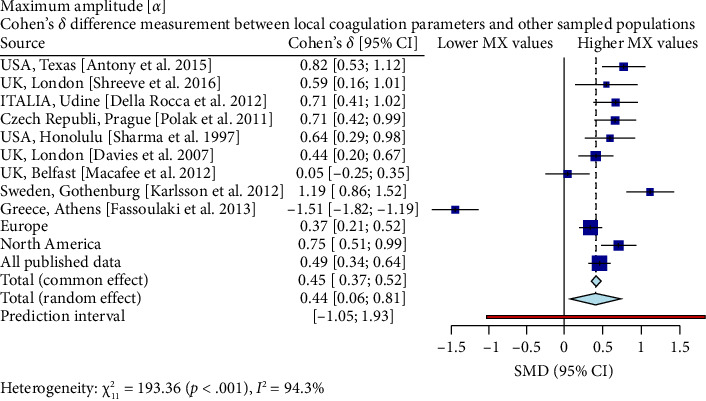
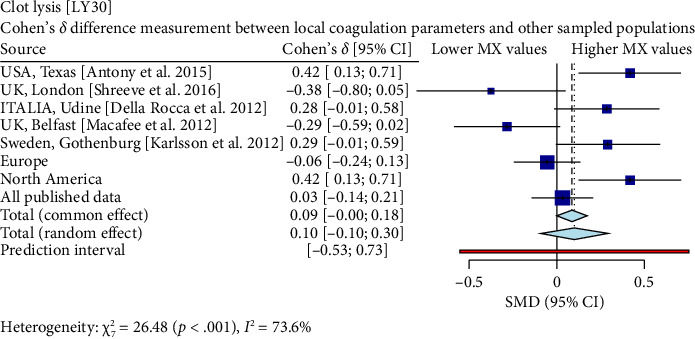
Objective: This prospective, descriptive, cross-sectional study aimed to establish kaolin-based thromboelastography reference values for previously known healthy third-trimester pregnancy patients. Methods: The study included 280 patients aged 18-38 years who were admitted to labor or scheduled for elective c-sections. Blood specimens collected via IV catheters were immediately mixed with reagents, placed in coagulation cups, and subjected to 60 min of testing at 37°C using a Haemonetics TEG 5000 system. The Hoffman regression method calculated the reference values; furthermore, effect size determination was done using Cohen's δ for comparison of data from other sources. Results: Patients had a median age of 26 (IQR 22-31), and their thromboelastography profile exhibited reference values for: R time (1-7 min), clot kinetics (1-2), angle (59°-82°), maximum amplitude (60-86 mm), and clot lysis at both 30 min (0%-6%) and 60 min (0%-8%). Results revealed significant differences in various thromboelastography parameters when comparing local patient cohorts against published reports, mainly European and North American counterparts. Shorter reaction times, enhanced clot kinetics, larger angles, and higher maximum amplitude, curve amplitude at 30 min, and amplitude at 60 min indicated distinct coagulation profiles and behaviors in the northeastern region of Mexico. Conclusion: Reference values for the Northern region of Mexico have been calculated and are characterized by a shorter clot reaction time, faster clot dynamics, higher angle values, overall greater curve amplitude, and no differences in enzymatic lysis activity compared to samples from other geographic regions.
Keywords: coagulation; goal-directed therapy; obstetric hemorrhage; reference values; thromboelastography; viscoelastic analysis.
Copyright © 2025 S. Alvarado-Ramos et al. Anesthesiology Research and Practice published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Lumbreras-Marquez M. I., Villela-Franyutti D., Reale S. C., Farber M. K. Coagulation Management in Obstetric Anesthesia. Current Anesthesiology Reports . 2022;12(2):266–276. doi: 10.1007/s40140-022-00517-1. - DOI
LinkOut - more resources
Full Text Sources
