

Delirium as a Determinant of Long-Term Cognitive Dysfunction in the Context of Post-intensive Care Syndrome: A Prospective Study in a Latin American Environment
- PMID: 40225547
- PMCID: PMC11994226
- DOI: 10.7759/cureus.80578
Delirium as a Determinant of Long-Term Cognitive Dysfunction in the Context of Post-intensive Care Syndrome: A Prospective Study in a Latin American Environment
Abstract
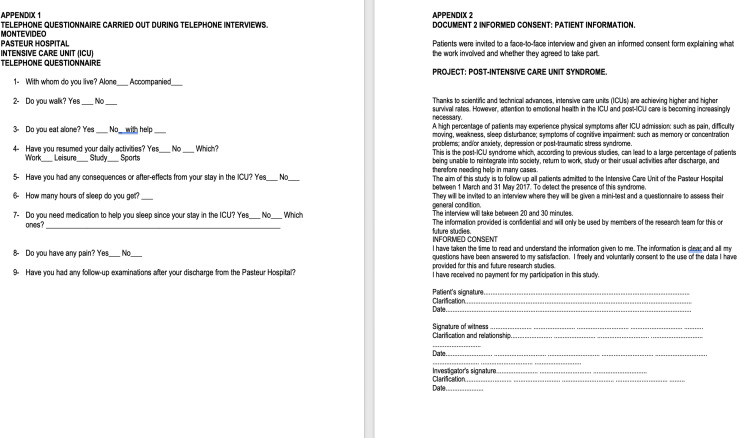
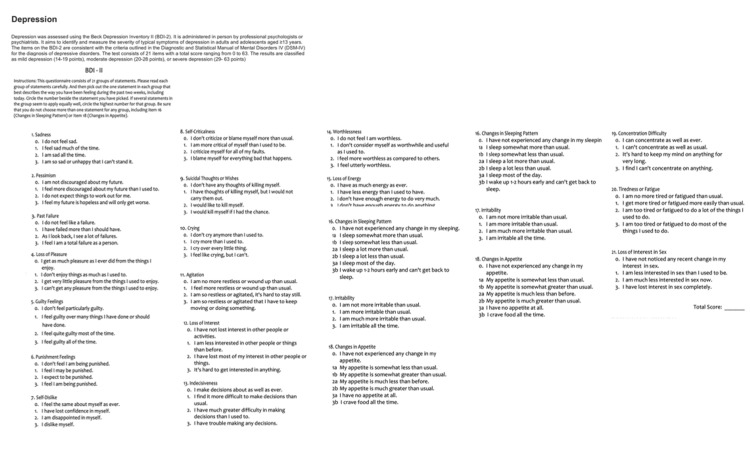
Introduction Cognitive dysfunction represents a major healthcare concern in the 21st century. Prolonged cognitive dysfunction and concomitant psychological and physical disorders in patients admitted to the intensive care unit (ICU) are components of the post-ICU syndrome (PICS). Notwithstanding the numerous published studies in this area, our work is the first to explore the relationship between PICS and delirium in the ICU in Uruguay. This research underscores the significance and potential of our study, which we believe will make a substantial contribution to this field of research in Latin America. Objectives The incidence rates of the cognitive, psychological, and physical sequelae constituting PICS were evaluated, and the relationships between these disorders and delirium in the ICU were studied. Methods This was a prospective cohort study in which patients were followed up for one year after admission to the ICU of Hospital Pasteur between 03/01/2017 and 05/31/2017. The pre-ICU condition of each patient was considered in the analysis. An initial telephone interview was conducted using the following scales: the Hamilton scale was used to assess anxiety, the Pfeiffer scale was used to assess cognitive impairment, and the Barthel scale was used to assess activities of daily living (ADLs). In a second face-to-face interview, the Mini-Mental State Examination (MMSE) and the Beck Depression Scale II (BDS-II) were used. Results Forty-three patients were divided into two groups: 15 (34%) with delirium in the ICU and 28 (66%) without delirium. The association of delirium with different sequelae was evaluated using the corresponding scales: Pfeiffer scale: Cognitive impairment was observed in 7/13 patients (53%) in the delirium group vs. 0/29 patients (0%) in the non-delirious group (p 0.001); MMSE score: Deterioration was observed in 6/7 patients (86%) in the delirium group vs. 1/7 patients (14%) in the non-delirious group (p 0.007). Cognitive impairment was found in 3/6 patients (50%) who presented with delirium in the ICU, while 1/8 patients (13%) who did not present with delirium experienced cognitive impairment (p = 0.036); Hamilton scale: Anxiety was found in 8/15 patients (57%) in the delirium group and 20/29 patients (68%) in the non-delirious group; BDS-II: Depression was found in 12/12 patients (100%) in the delirium group vs. 27/29 patients (93%) in the non-delirious group (p 0.57). Barthel scale: Dependence on others for ADLs was observed in 3/15 patients (20%) in the delirium group vs. 4/29 patients (14%) in the non-delirious group (p = 0.23). Conclusions Cognitive impairment was observed to be associated with delirium in the ICU, opening new avenues for research and possible treatment options. Although dependence on activities of daily living (ADLs) was more common in the delirium group, the difference between the two groups was not significant, highlighting the need for further research to understand the whole picture. Rates of anxiety and depression after ICU stay were also similar between the two groups, providing a baseline for comparison and informing future studies. The study highlights the urgent need for delirium-specific interventions in the ICU to address cognitive dysfunction and improve long-term outcomes in critically ill patients.
Keywords: cam-icu; cognitive; cognitive impairment; delirium; medical intensive care unit (micu); physical sequelae; post intensive care; psychological.
Copyright © 2025, Mesa et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Pasteur Hospital issued approval Minutes 29/006/3/696/2017/0/0. The Research Ethics Committee of Hospital Pasteur, State Administration of Health Services (ASSE), Montevideo, Uruguay, approved the study (Minutes 29/006/3/696/2017/0/0). All enrolled patients signed an informed consent form. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures





References
-
- Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders' conference. Needham DM, Davidson J, Cohen H, et al. Crit Care Med. 2012;40:502–509. - PubMed
-
- Combination of delirium and coma predicts psychiatric symptoms at twelve months in critically ill patients: A longitudinal cohort study. Miyamoto K, Shibata M, Shima N, et al. J Crit Care. 2021;63:76–82. - PubMed
LinkOut - more resources
Full Text Sources