

Personalized prediction for recurrence of cystitis glandularis: insights from SHAP and machine learning models
- PMID: 40226087
- PMCID: PMC11986474
- DOI: 10.21037/tau-2024-665
Personalized prediction for recurrence of cystitis glandularis: insights from SHAP and machine learning models
Abstract
Background: Cystitis glandularis (CG) is a rare urological condition characterized by glandular metaplasia of the bladder mucosa. Recurrence following transurethral resection (TUR) is a significant clinical challenge. Traditional predictive models often fail to capture the complexity of the data, resulting in insufficient accuracy. In contrast, machine learning (ML) has demonstrated substantial potential in medical prediction by identifying and analyzing complex patterns that are undetectable by conventional methods. This study aims to develop and evaluate an interpretable ML model to predict recurrence after TUR for CG, thereby improving clinical decision-making and patient outcomes.
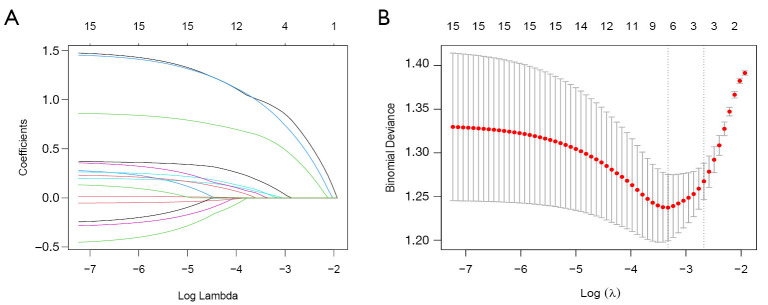
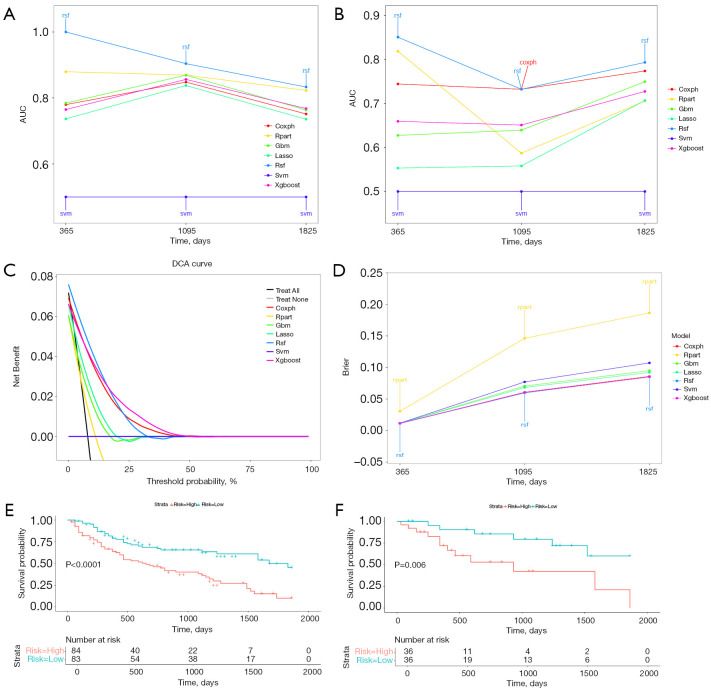
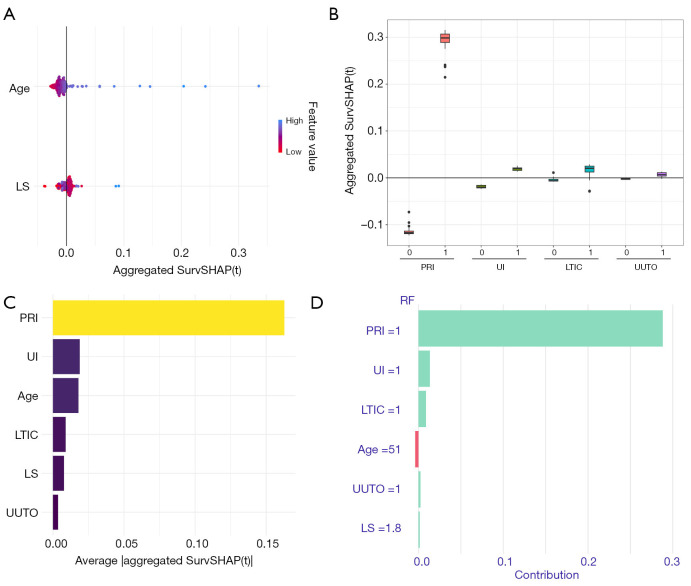
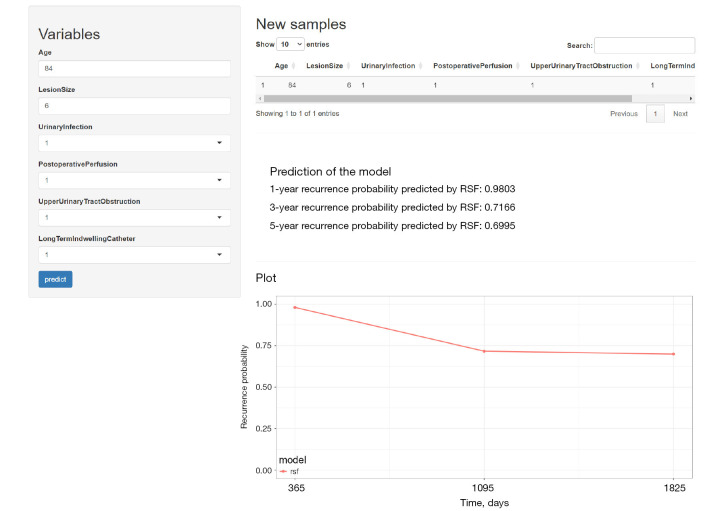
Methods: We analyzed predictors of recurrence using the least absolute shrinkage and selection operator (LASSO) and multivariate logistic regression. We developed and tested seven ML-based models: Cox proportional hazards model (CoxPH), LASSO regression, decision tree (rpart), random survival forest (RSF), gradient boosting machine (GBM), support vector machine (SVM), and extreme gradient boosting (XGBoost). Participants were diagnosed with CG by pathology following TUR and treated from 2012 to 2018. Model discrimination was assessed using the receiver operating characteristic (ROC) curve and area under the ROC curve (AUC), while model preference was evaluated through the Brier score (BS). Decision curve analysis (DCA) was used for model comparison. The SHapley Additive exPlanations (SHAP) method was employed for interpretation, providing insights into recurrence prediction and prevention strategies. Finally, user-friendly platform was developed, allowing users to predict CG recurrence by entering feature values into designated text boxes on the webpage.
Results: The RSF model demonstrated the best performance in predicting recurrence, as indicated by superior ROC, DCA, and BS metrics. In SHAP, postoperative regular instillation (PRI) contributed the most to model construction.
Conclusions: The RSF model effectively predicts CG recurrence, offering a framework for individualized treatment strategies. PRI was identified as the most significant risk factor influencing recurrence.
Keywords: Cystitis glandularis (CG); SHapley Additive exPlanations (SHAP); machine learning (ML); online platform; prediction model.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tau.amegroups.com/article/view/10.21037/tau-2024-665/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources