

Automated collateral assessment restricted to the hypoperfused area for distal vessel occlusions in ischemic stroke
- PMID: 40227346
- PMCID: PMC12417235
- DOI: 10.1007/s00330-025-11442-2
Automated collateral assessment restricted to the hypoperfused area for distal vessel occlusions in ischemic stroke
Abstract
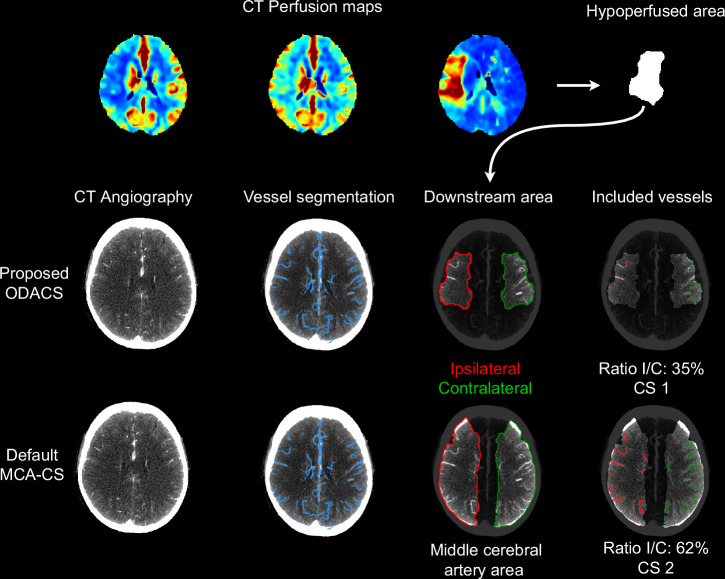
Objectives: This study aims to: (1) develop and evaluate a quantitative assessment of collateral status in the downstream area of an occluded intracranial artery in acute ischemic stroke and compare this method to middle cerebral artery (MCA)-based assessment; (2) determine the agreement between the automated occlusion-downstream area collateral score (ODACS) and expert raters' assessments, and compare this to inter-rater agreement.
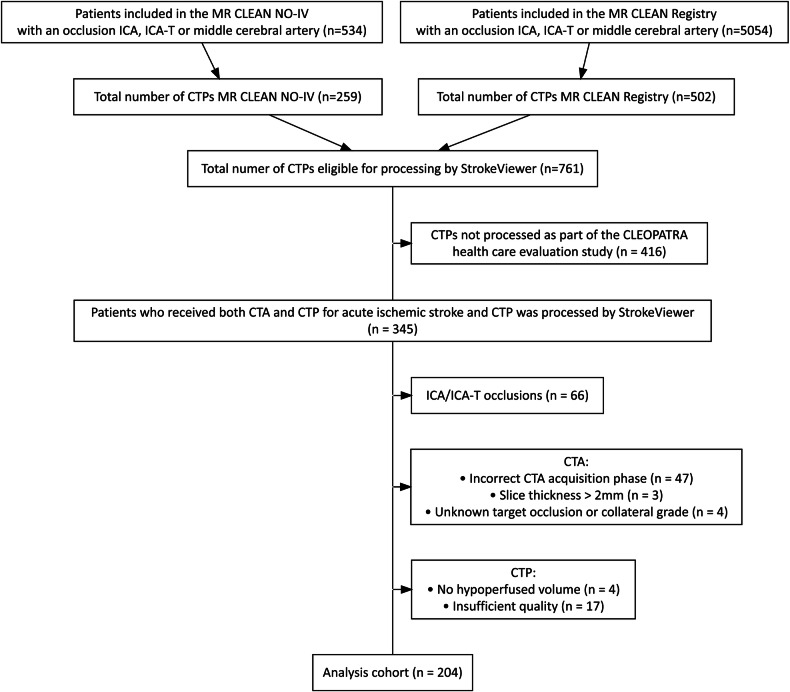
Methods: Patients from MR CLEAN-NO IV and MR CLEAN Registry with a proximal M1, distal M1, or M2 occlusion were included. Using the hypoperfused area from CT perfusion (CTP) as a proxy for the occlusion-downstream territory and automated vessel segmentations from CT angiography (CTA), ODACS is calculated as the vessel volume ratio between downstream ipsilateral and its contralateral regions. ODACS was compared to a whole MCA-territory approach and evaluated against visual scoring by two expert raters that visually estimated ODACS using CTA and CTP, and their inter-rater agreement.
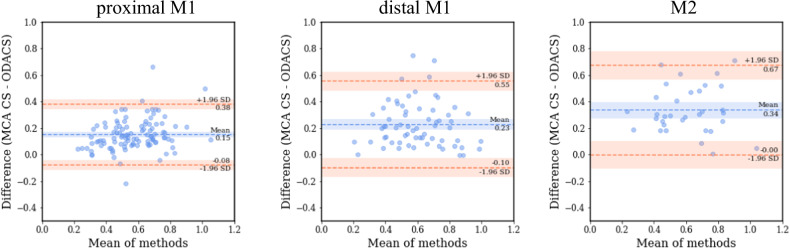
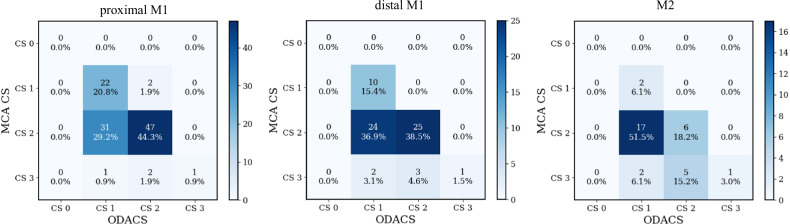
Results: The study included 204 patients with a proximal M1 (52%), distal M1 (32%), or M2 (16%) occlusion. ODACS yielded lower collateral scores than MCA-based scoring for all occlusion locations, with larger differences in more distal occlusions. For M2 occlusions, 58% of patients shifted from good (> 50%) to poor (≤ 50%) collateral filling of the occluded territory using ODACS. Moderate (weighted Cohen's kappa κ = 0.45) inter-rater agreement and fair (κ = 0.35) to moderate (κ = 0.51) ODACS-rater agreement were observed.
Conclusions: ODACS yields lower collateral scores compared to MCA-based scoring and is comparable to scores from expert raters.
Key points: Question CT angiography-based collateral assessment in the MCA territory is inadequate to assess the collateral status in patients with distal vessel occlusions. Findings Our automated ODACS revealed lower collateral scores than traditional whole-territory assessment, especially in distal vessel occlusions. Clinical relevance The more precise evaluation of affected brain territories through automated occlusion-downstream area assessments prevents an overestimation of collateral status in distal occlusions, which could lead to improved patient selection and treatment decisions in acute stroke care.
Keywords: Brain; Collateral circulation; Computed tomography angiography; Perfusion imaging; Stroke.
© 2025. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is H.A. Marquering. Conflict of interest: The authors of this manuscript declare relationships with the following companies: Nicolab B.V. Statistics and biometry: No complex statistical methods were necessary for this paper. Informed consent: Both written informed consent was obtained from all subjects (patients) in this study and Written informed consent was waived by the Institutional Review Board. The ethics committee waived the necessity of written informed consent for the MR CLEAN Registry; written informed consent was obtained for all patients in MR CLEAN-NO IV. Ethical approval: Institutional Review Board approval was obtained. Study subjects or cohorts overlap: Our study uses data from the CONTRAST consortium ( https://www.contrast-consortium.nl ), specifically from the MR CLEAN NO-IV trial and MR CLEAN Registry, which have been extensively employed in various research studies. We have included references to the two main papers that detail the results from the MR CLEAN NO-IV trial and MR CLEAN Registry in our submission: LeCouffe NE, Kappelhof M, Treurniet KM et al (2021) A randomized trial of intravenous alteplase before EVT for stroke. N Engl J Med 385:1833–1844. Compagne KC, Kappelhof M, Hinsenveld WH et al (2022) Improvements in EVT for acute ischemic stroke: a longitudinal study in the MR CLEAN registry. Stroke 53:1863–1872. Additionally, we want to note that the datasets from the consortium have been widely used in other studies. The CONTRAST consortium, however, assures that there is no overlap between research proposals and manuscripts. Methodology: Retrospective Diagnostic or prognostic study Multicenter study
Figures

References
-
- Boers AMM, Sales Barros R, Jansen IGH et al (2017) Quantitative collateral grading on CT angiography in patients with acute ischemic stroke. Lect Notes Comput Sci 10555 LNCS:176–184. 10.1007/978-3-319-67564-0_18
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
