

Endoscopic Submucosal Dissection (ESD) for the Management of Fibrotic Non-Lifting Colorectal Lesions (NLCLs): Results from a Large Multicenter Retrospective Study
- PMID: 40227777
- PMCID: PMC11987842
- DOI: 10.3390/cancers17071242
Endoscopic Submucosal Dissection (ESD) for the Management of Fibrotic Non-Lifting Colorectal Lesions (NLCLs): Results from a Large Multicenter Retrospective Study
Abstract
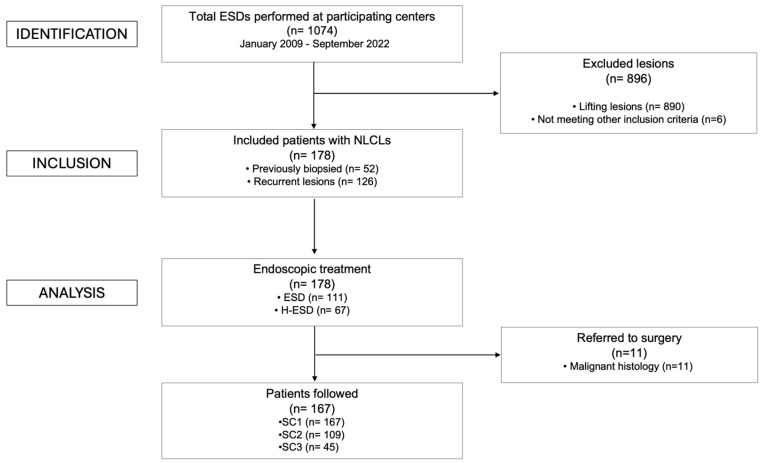
Background/Objectives: The management of non-lifting colorectal lesions (NLCLs), often resulting from previous unsuccessful treatments or biopsies, remains challenging due to submucosal fibrosis that prevents adequate lifting. Endoscopic submucosal dissection (ESD) is a viable option for achieving complete resection in such cases. However, when standard ESD is not feasible, conversion to hybrid ESD (H-ESD) has been proposed as a rescue strategy. This study aimed to assess ESD's feasibility, effectiveness, and safety for NLCLs, including cases requiring conversion to H-ESD, when performed by experienced endoscopists in tertiary referral centers. Methods: In this multicenter retrospective study, data from patients with NLCLs treated by ESD/H-ESD between January 2009 and September 2022 were analyzed. The primary endpoint was the recurrence rate (RR). Secondary endpoints included the adverse event (AE) rate, technical success (TS) rate (en bloc resection regardless of technique), complete resection (CR), curative resection (cR) rates, and surgical intervention rate. Predictors of ESD technical success were identified. Results: In total, 178 patients with NLCLs were included (52 previously biopsied, 126 recurrent after previous resection). ESD was used in 111 (62.4%) and H-ESD in 67 (37.6%) cases. During a median follow-up of 373 days (IQR 540), the overall RR was 3.6%. The overall AE rate was 13.4%, and perforation was the most frequent (8.4%). All AEs were successfully managed endoscopically. The TS rate was 71.9%, significantly higher in previously biopsied lesions compared to recurrent ones (78.8% vs. 55.6%, p = 0.04). On multivariate analysis, rectal location (p < 0.001), F1 fibrosis (p = 0.026), and previously biopsied lesions (p = 0.006) predicted ESD TS without the need for conversion to H-ESD. Conclusions: ESD/H-ESD is feasible and safe for NLCLs when performed by experienced operators, with low RR amenable to endoscopic treatment. Previously biopsied lesions, rectal location, and low fibrosis predict ESD TS.
Keywords: EMR; ESD; NLCL; colorectal; hybrid; no-lifting; polyps; recurrent.
Conflict of interest statement
S.D. has served as a speaker, consultant, and advisory board member for Schering-Plough, AbbVie, Actelion, Alphawasserman, AstraZeneca, Cellerix, Cosmo Pharmaceuticals, Ferring, Genentech, Grunenthal, Johnson and Johnson, Millenium Takeda, MSD, Nikkiso Europe GmbH, Novo Nordisk, Nycomed, Pfizer, Pharmacosmos, UCB Pharma, and Vifor. The other authors declare no conflicts of interest.
Figures

Similar articles
-
Underwater endoscopic submucosal dissection and hybrid endoscopic submucosal dissection as rescue therapy in difficult colorectal cases.Endosc Int Open. 2022 Sep 14;10(9):E1225-E1232. doi: 10.1055/a-1882-4306. eCollection 2022 Sep. Endosc Int Open. 2022. PMID: 36118634 Free PMC article.
-
AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States.Clin Gastroenterol Hepatol. 2019 Jan;17(1):16-25.e1. doi: 10.1016/j.cgh.2018.07.041. Epub 2018 Aug 2. Clin Gastroenterol Hepatol. 2019. PMID: 30077787 Review.
-
Efficacy of hybrid endoscopic submucosal dissection (ESD) as a rescue treatment in difficult colorectal ESD cases.Dig Endosc. 2017 Apr;29 Suppl 2:45-52. doi: 10.1111/den.12863. Dig Endosc. 2017. PMID: 28425649
-
Safety and efficacy of endoscopic submucosal dissection for rectal neoplasia: a multicenter North American experience.Endosc Int Open. 2019 Dec;7(12):E1714-E1722. doi: 10.1055/a-1010-5663. Epub 2019 Dec 2. Endosc Int Open. 2019. PMID: 31803823 Free PMC article.
-
Endoscopic submucosal dissection for colorectal neoplasia: outcomes and predictors of recurrence.Endosc Int Open. 2022 Jan 14;10(1):E127-E134. doi: 10.1055/a-1551-3058. eCollection 2022 Jan. Endosc Int Open. 2022. PMID: 35047343 Free PMC article. Review.
Cited by
-
Endoscopic resection of colorectal laterally spreading tumors: Clinicopathologic characteristics and risk factors for treatment outcomes.World J Gastrointest Endosc. 2025 Jun 16;17(6):106412. doi: 10.4253/wjge.v17.i6.106412. World J Gastrointest Endosc. 2025. PMID: 40547554 Free PMC article.
References
-
- Kobayashi N., Saito Y., Sano Y., Uragami N., Michita T., Nasu J., Matsuda T., Fu K., Fujii T., Fujimori T., et al. Determining the Treatment Strategy for Colorectal Neoplastic Lesions: Endoscopic Assessment or the Non-Lifting Sign for Diagnosing Invasion Depth? Endoscopy. 2007;39:701–705. doi: 10.1055/s-2007-966587. - DOI - PubMed
-
- Cecinato P., Lisotti A., Azzolini F., Lucarini M., Bassi F., Fusaroli P., Sassatelli R. Left Colonic Localization, Non-Granular Morphology, and Pit Pattern Independently Predict Submucosal Fibrosis of Naïve Colorectal Neoplasms before Endoscopic Submucosal Dissection. Surg. Endosc. 2023;37:3037–3045. doi: 10.1007/s00464-022-09828-0. - DOI - PubMed
-
- Sferrazza S., Maida M., Calabrese G., Facciorusso A., Fuccio L., Frazzoni L., Maselli R., Repici A., Di Mitri R., Santos-Antunes J. The Derivation and External Validation of a Fibrosis Risk Model for Colorectal Tumours Undergoing Endoscopic Submucosal Dissection. J. Clin. Med. 2024;13:4517. doi: 10.3390/jcm13154517. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
