

Effectiveness of kinesiotaping for lymphatic drainage after bilateral total knee arthroplasty: A randomized controlled trial
- PMID: 40228285
- PMCID: PMC11999401
- DOI: 10.1097/MD.0000000000041971
Effectiveness of kinesiotaping for lymphatic drainage after bilateral total knee arthroplasty: A randomized controlled trial
Abstract
Background: The effectiveness of kinesiotape for lymphatic drainage has been studied by comparing groups of patients with unilateral total knee arthroplasty (TKA). Studying its impact on persons with bilateral TKA may give a more accurate assessment of effectiveness. The purpose of this study was to evaluate the effectiveness of kinesiotaping for lymphatic drainage in reducing postoperative edema and pain and improving the knee range of motion (ROM) of adults with bilateral TKA.
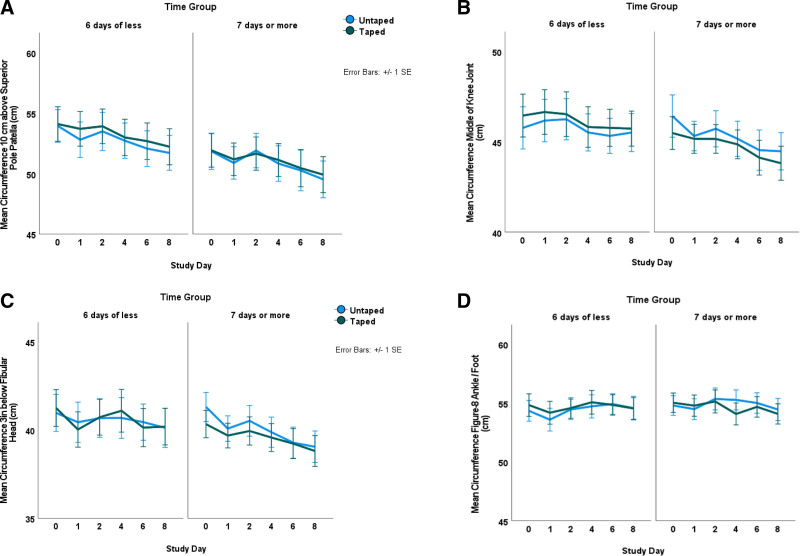
Methods: Using a randomized controlled trial, mixed-model design, 52 eligible adults began standard inpatient rehabilitation 3 to 13 days after bilateral TKA. Kinesiotape for lymphatic drainage was applied to 1 randomly selected leg of 52 consenting participants (mean age = 68.1 years, standard deviation = 7.6; 62% female). Leg circumferences, active and active-assistive knee ROM, and Numerical Pain Rating were measured bilaterally at baseline (before kinesiotaping) and on study days 1, 2, 4, 6, and 8 with kinesiotape. A mixed-model analysis of variance examined interactions among within-subjects (day, leg taped) and between-subjects (time between surgery and kinesiotape application) factors.
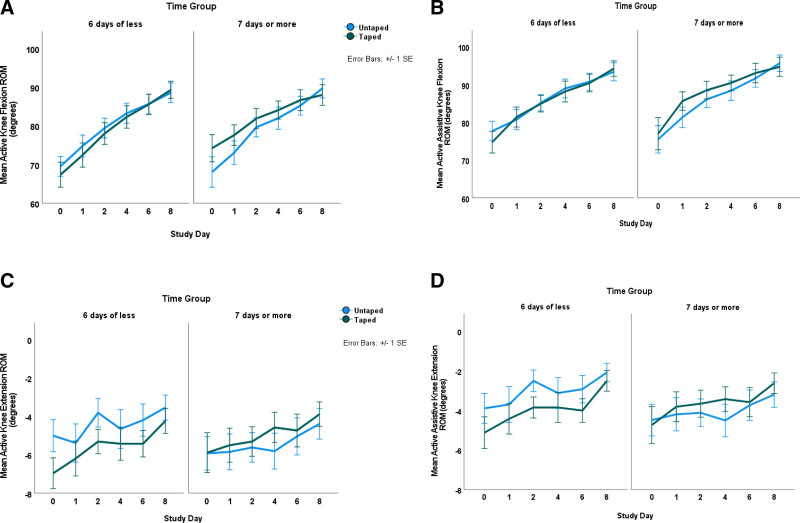
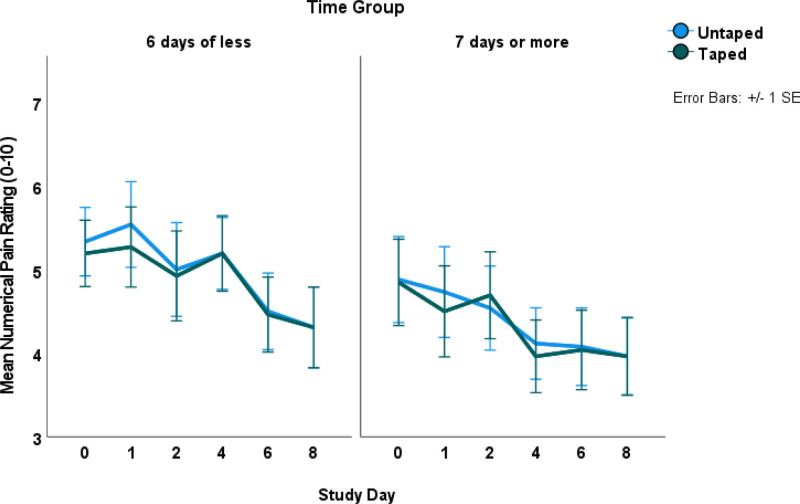
Results: Interactions of day by taped leg by time group for knee active flexion (F = 4.32, P =.006, η2 =0.076) were attributed to higher baseline knee flexion of the taped leg for persons with 7 days or more between surgery and kinesiotaping (n = 25; mean knee flexion = 74.9°, standard deviation = 17.8) compared with the taped legs of the 6 days or less group (n = 27; mean knee flexion = 66.9°, standard deviation = 16.3). This interaction also reflects significant improvements from days 1 to 2 for the taped leg of the 6-day or less group (MeanDiffDay1-2 = 5.6°, standard error = 1.5, P =.008) and improvement of the untaped leg of the 7-day or more group (MeanDiffDay1-2 = 6.7°, standard error = 1.7, P =.005). No significant day-by-leg or day-by-leg-by-time group interactions occurred for circumferences, Numerical Pain Rating, and active knee extension and active-assistive knee flexion and extension.
Conclusions: Kinesiotaping for lymphatic drainage does not augment standard inpatient rehabilitation for edema control, ROM improvement, and pain remission after bilateral TKA.
Trial registration: ClinicalTrials.gov NCT05013879.
Keywords: edema; inpatients; kinesiotape; total knee arthroplasty; total knee replacement.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures

Similar articles
-
Effects of combining manual lymphatic drainage and Kinesiotaping on pain, edema, and range of motion in patients with total knee replacement: a randomized clinical trial.Int J Rehabil Res. 2020 Sep;43(3):240-246. doi: 10.1097/MRR.0000000000000417. Int J Rehabil Res. 2020. PMID: 32459670 Clinical Trial.
-
Does an Elastic Compression Bandage Provide Any Benefit After Primary TKA?Clin Orthop Relat Res. 2019 Jan;477(1):134-144. doi: 10.1097/CORR.0000000000000459. Clin Orthop Relat Res. 2019. PMID: 30794237 Free PMC article. Clinical Trial.
-
Effect of Manual Lymphatic Drainage After Total Knee Arthroplasty: A Randomized Controlled Trial.Arch Phys Med Rehabil. 2016 May;97(5):674-82. doi: 10.1016/j.apmr.2016.01.006. Epub 2016 Jan 30. Arch Phys Med Rehabil. 2016. PMID: 26829760 Clinical Trial.
-
Effects of kinesiotaping during early post-operative rehabilitation in individuals who underwent a total knee arthroplasty: A systematic review and meta-analysis of randomized control trials.Clin Rehabil. 2024 Jun;38(6):732-748. doi: 10.1177/02692155241230894. Epub 2024 Feb 6. Clin Rehabil. 2024. PMID: 38321770
-
Effect of Postoperative Kinesio Taping on Knee Edema, Pain, and Range of Motion After Total Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Randomized Clinical Trials.JBJS Rev. 2024 Mar 15;12(3). doi: 10.2106/JBJS.RVW.23.00221. eCollection 2024 Mar 1. JBJS Rev. 2024. PMID: 38489396
References
-
- Singh JA, Shaohua Y, Lang C, Cleveland JD, Yu S, Chen L. Rates of total joint replacement in the United States: future projections to 2020-2040 using the national inpatient sample. J Rheumatol. 2019;46:1134–40. - PubMed
-
- Dubin JA, Bains SS, Hameed D, et al. . Projected volume of primary total joint arthroplasty in the USA from 2019 to 2060. Eur J Orthop Surg Traumatol. 2024;34:2663–70. - PubMed
-
- Dubin JA, Bains SS, Monárrez R, et al. . The effect of insurance type on length of stay following total knee arthroplasty. J Arthroplasty. 2025;40:75–9. - PubMed
-
- Centers for Medicare and Medicaid Services. Total knee arthroplasty (TKA) removal from the medicare inpatient-only (IPO) list and application of the 2-midnight rule. American Heart Association. https://www.cms.gov/files/document/se18018pdf#:~:text=The%20Centers%20fo.... Accessed January 23, 2025.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
