

The supramolecular polymer-related signature predicts prognosis and indicates immune microenvironment infiltration in gastric cancer
- PMID: 40228435
- PMCID: PMC12017930
- DOI: 10.1016/j.clinsp.2025.100641
The supramolecular polymer-related signature predicts prognosis and indicates immune microenvironment infiltration in gastric cancer
Abstract
Background: Gastric Cancer (GC) remains a leading global cause of cancer mortality, underscoring the urgent need for advanced prognostic tools. This study aimed to construct and evaluate a prognostic risk signature based on Supramolecular Polymer-Related Genes (SPRGs) in gastric cancer.
Methods: The authors downloaded data from TCGA-STAD, GEO, and CCLE databases for patients with GC and validation cohorts. Through consensus clustering, Cox proportional hazards models, LASSO Cox regression, and nomogram development, the authors identified and constructed a GC Prognostic risk Index (SPI). Additionally, the authors conducted drug sensitivity analysis and immune landscape assessment. Functional evaluations were conducted through colony formation, transwell invasion, and wound healing assays.
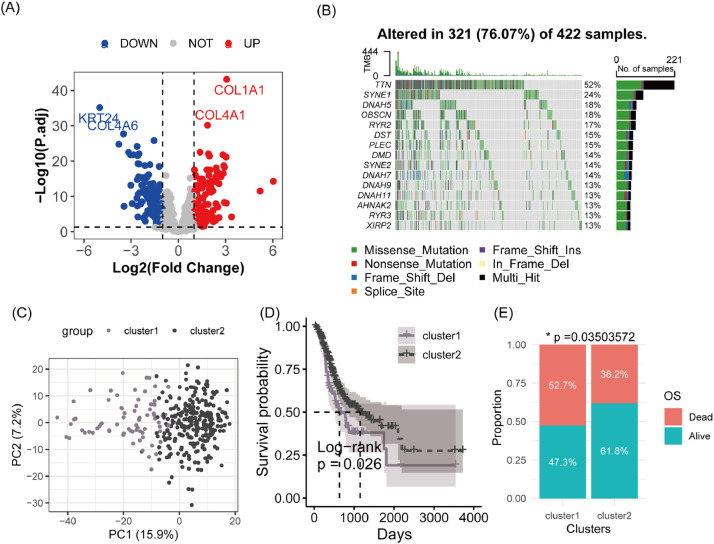
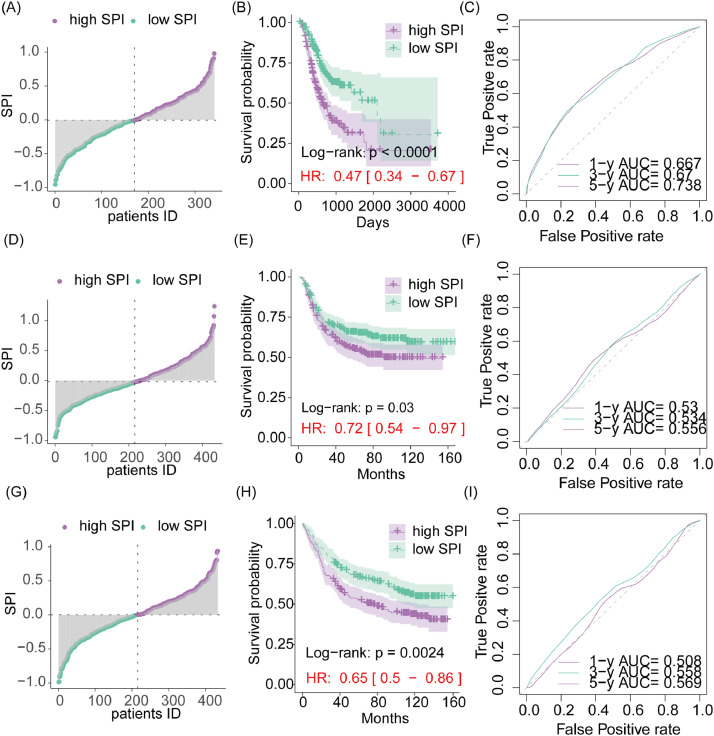
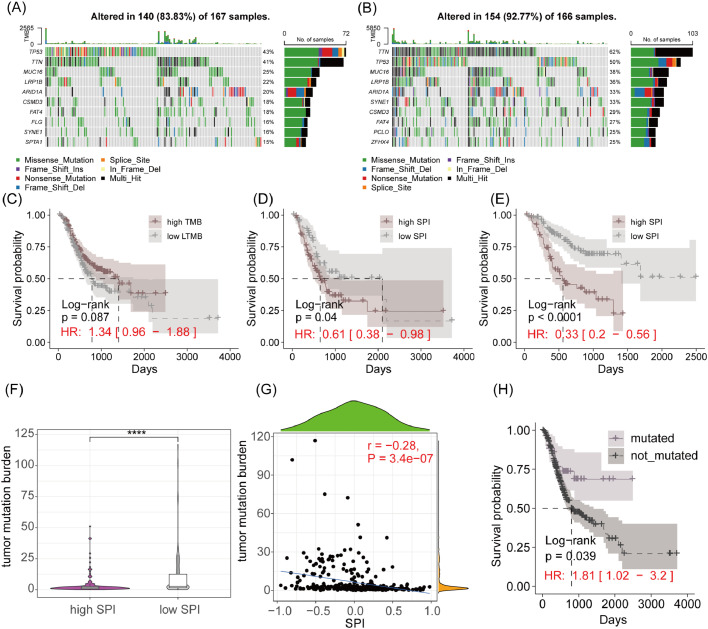
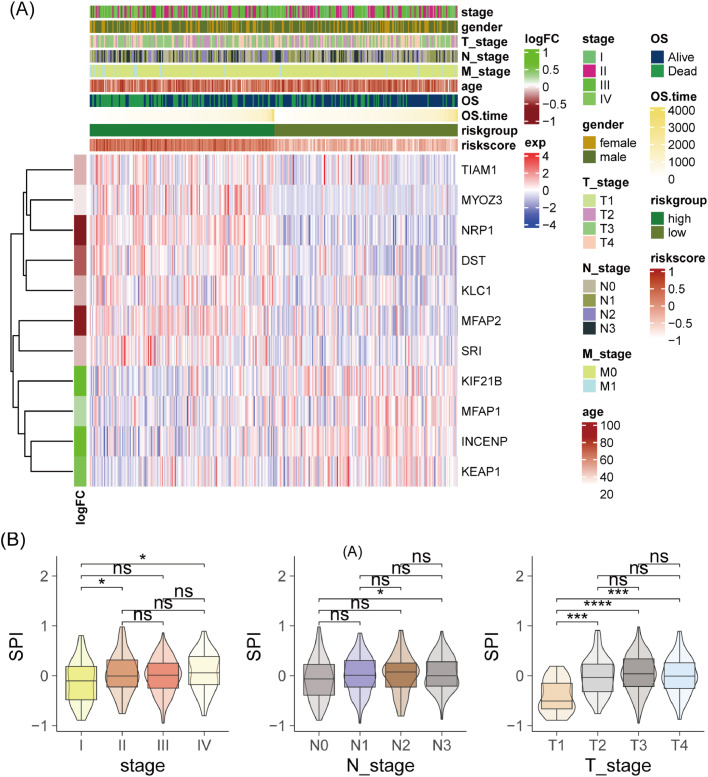
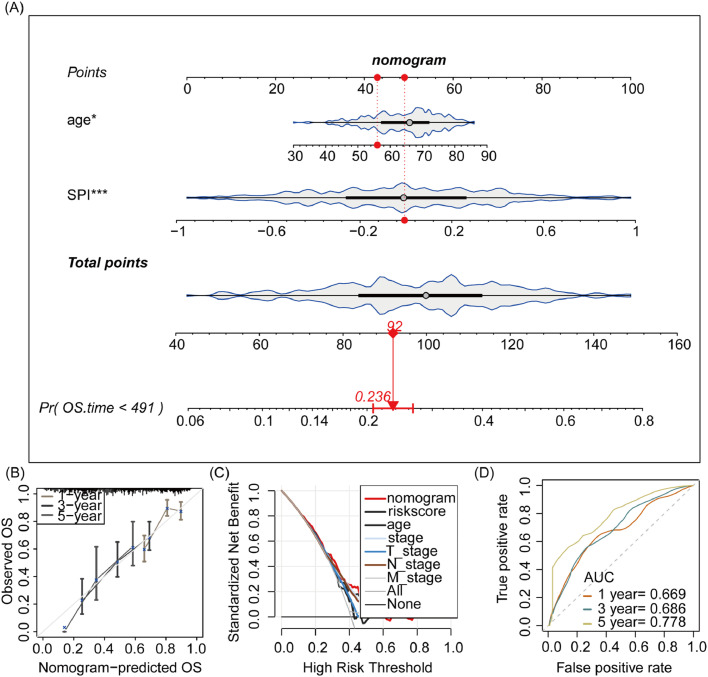
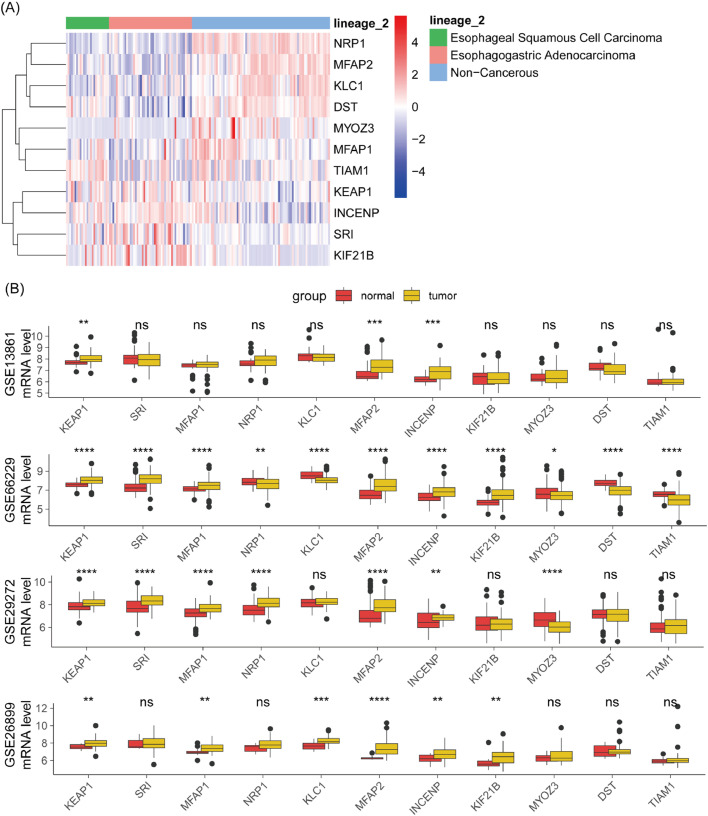
Results: The authors identified that 182 SPRGs were significantly upregulated and 226 were downregulated in gastric cancer. Consensus clustering revealed two molecular subtypes, with cluster 1 having significantly lower overall survival compared to cluster 2. SPI effectively distinguished high-risk and low-risk patients across all cohorts. Furthermore, SPI was associated with tumor stage, lymph node metastasis, and tumor size, and could predict drug sensitivity in GC patients. Immune landscape analysis showed higher infiltration of naïve B cells, M2 macrophages, and activated NK cells in high-SPI patients. A nomogram model for GC prognosis using SPI and patient age was developed. KLC1 knockdown significantly suppressed GC cell proliferation, while markedly attenuating metastatic potential and invasion capacity.
Conclusion: This study constructed a prognostic risk signature based on SPRGs in gastric cancer, which is closely related to clinical pathological features, drug sensitivity, and immune landscape, providing new insights for personalized treatment.
Keywords: Gastric cancer; Immune landscape; LASSO; Nomogram; Supramolecular polymer.
Copyright © 2025. Published by Elsevier España, S.L.U.
Conflict of interest statement
Conflicts of interest The authors declare no conflicts of interest.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
