

Alcohol related hepatitis in intensive care units: clinical and biological spectrum and mortality risk factors: a multicenter retrospective study
- PMID: 40229464
- PMCID: PMC11996726
- DOI: 10.1186/s13613-025-01450-2
Alcohol related hepatitis in intensive care units: clinical and biological spectrum and mortality risk factors: a multicenter retrospective study
Abstract
Background: Alcohol related hepatitis is responsible for high morbidity and mortality, but little is known about the management of patients with hepatitis specifically in intensive care units (ICU).
Methods: Retrospective study including patients with alcohol related hepatitis hospitalized in 9 French ICUs (2006-2017). Alcohol related hepatitis was defined histologically or by an association of clinical and biological criteria according to current guidelines.
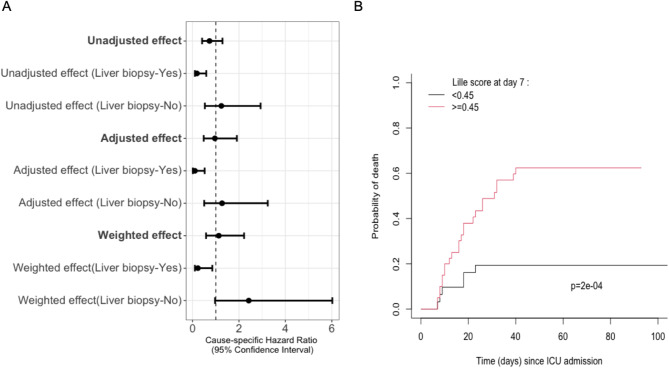
Results: 187 patients (median age: 53 [43-60]; male: 69%) were included. A liver biopsy was performed in 51% of cases. Patients were admitted for impaired consciousness (71%), sepsis (64%), shock (44%), respiratory failure (37%). At admission, median SOFA and MELD scores were 10 [7-13] and 31 [26-40] respectively. 63% of patients received invasive mechanical ventilation, 62% vasopressors, and 36% renal replacement therapy. 66% of patients received corticosteroids, and liver transplantation was performed in 16 patients (8.5%). ICU and in-hospital mortality were 37% and 53% respectively. By multivariate analysis, ICU mortality was associated with SOFA score (without total bilirubin) (SHR 1.08 [1.02-1.14] per one-point increase), arterial lactate (SHR 1.08 [1.03-1.13] per 1 mmol/L) and MELD score (SHR 1.09 [1.04-1.14] per 1 point), while employment was associated with increased survival (HR 0.49 [0.28-0.86]). After propensity score weighting, the use of corticosteroids did not affect ICU mortality in the overall population but had a beneficial effect in the subgroup of patients with histological proof. Patient prognosis was also better in responders assessed by Lille score at day 7 (OR 6.67 [2.44-20.15], p < 0.001).
Conclusion: Alcohol related hepatitis is a severe condition leading to high mortality in ICU patients. Severity of organ failure at admission are mortality risk factors. Outcome was significantly better in responders to corticosteroids therapy according to Lille score. Early referral to tertiary centers to discuss liver transplantation should more widely be considered.
Keywords: Alcohol related hepatitis; Alcoholic hepatitis; Corticosteroids; Intensive care; Lille score; Liver transplantation; Mortality.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The French Society of Intensive Care ethics committee approved the study (HAA-MIR reference CE SRLF 23 − 008). Written informed consent was not required, in compliance with French law on retrospective studies of anonymized data. All local medico-administrative data bases are declared to the Commission Nationale Informatique et Liberté (CNIL). Competing interests: The authors declare that they have no competing interests.
Figures


References
-
- Mathurin P, Mendenhall CL, Carithers RL, Ramond MJ, Maddrey WC, Garstide P, et al. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis (AH): individual data analysis of the last three randomized placebo controlled double blind trials of corticosteroids in severe AH. J Hepatol Avr. 2002;36(4):480–7. - DOI - PubMed
LinkOut - more resources
Full Text Sources
