

Accuracy of non-invasive measurement of cardiac output using electrical cardiometry in preterm infants during the transitional period: A comparison with transthoracic Doppler echocardiography
- PMID: 40229586
- PMCID: PMC11996928
- DOI: 10.1007/s00431-025-06132-6
Accuracy of non-invasive measurement of cardiac output using electrical cardiometry in preterm infants during the transitional period: A comparison with transthoracic Doppler echocardiography
Abstract
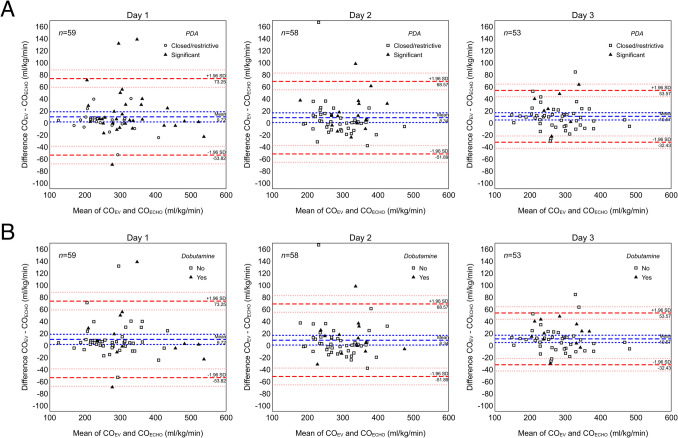
This prospective observational study aimed to assess the agreement of cardiac output measurements obtained with transthoracic echocardiography (COECHO) and electrical velocimetry (COEV) and the impact of relevant variables on COEV accuracy in preterm infants during the transitional period. Simultaneous measurements of COEV and COECHO were performed in preterm infants < 32 weeks' gestation and/or < 1500 g during the first 72 h of life. Bland-Altman analysis was performed and bias and mean percentage error (MPE) were calculated. The impact of a hemodynamically significant duct (hsPDA), ongoing cardiovascular drugs and ventilatory support was also assessed using a generalized least squares random-effects model. A total of 170 pairs of COEV-COECHO measurements were obtained from 65 preterm neonates. Mean bias was 9.7 ml/kg/min (95%CI 1.3-18.2) on day 1, 8.3 ml/kg/min (95%CI 0.3-16.4) on day 2, and 10.6 ml/kg/min (95%CI 4.5-16.6) on day 3 of life. The corresponding MPE was 7.2% (95%CI 4.8-10.6%), 7.5% (95%CI 4.7-12.8%) and 7.0% (95%CI 5.4-9.1%), respectively. A COEV overestimation was observed in the presence of hsPDA (mean bias = 17.0 ml/kg/min, 95%CI 7.1-30.8, p = 0.003) and during dobutamine treatment (mean bias = 12.5 ml/kg/min, 95%CI 1.5-22.4, p = 0.018). No significant differences were observed according to dopamine administration and respiratory support modality.
Conclusion: Although a slight overestimation may occur during inotropic treatments and in the presence of a hsPDA, this study shows an acceptable accuracy and precision of COEV in preterm infants during postnatal transition, thus supporting the role for EV monitoring in this critical phase.
What is known: • Electrical velocimetry allows a continuous and non-invasive monitoring of cardiac output (CO) in the neonatal population. • Available data comparing the accuracy of electrical velocimetry against transthoracic echocardiography for CO assessment in preterm infants are still controversial.
What is new: • The present data report a satisfactory accuracy of electrical velocimetry for CO assessment, with low bias and mean percentage error when compared to echocardiographic CO measurements. • Inotropic treatment with dobutamine and a hemodynamically significant duct may be associated with a slight but significant overestimation of CO measurements by electrical velocimetry.
Keywords: Accuracy; Echocardiography; Electrical velocimetry; Non-invasive cardiac output monitoring; Patent Ductus arteriosus; Preterm infants.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This is a sub-analysis of the NEO-ICM study, approved by the Ethics Committee of S. Orsola-Malpighi Hospital, Bologna, Italy (328/2017/O/Oss). Consent to participate: The consent for participation was obtained from the parents or legal guardians of the enrolled infants. Consent for publication: N/A. Conflict of interest: The authors declare no competing interests.
Figures
Similar articles
-
Electrical Cardiometry to Monitor Cardiac Output in Preterm Infants with Patent Ductus Arteriosus: A Comparison with Echocardiography.Neonatology. 2017;112(3):231-237. doi: 10.1159/000475774. Epub 2017 Jul 14. Neonatology. 2017. PMID: 28704819
-
Comparison of Cardiac Output Measurement by Electrical Velocimetry with Echocardiography in Extremely Low Birth Weight Neonates.Neonatology. 2022;119(1):18-25. doi: 10.1159/000519713. Epub 2021 Nov 1. Neonatology. 2022. PMID: 34724661
-
[Clinical study of neonatal cardiac output measurement methods].Zhonghua Er Ke Za Zhi. 2013 Jan;51(1):58-63. Zhonghua Er Ke Za Zhi. 2013. PMID: 23527933 Chinese.
-
Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis.J Clin Monit Comput. 2020 Jun;34(3):433-460. doi: 10.1007/s10877-019-00330-y. Epub 2019 Jun 7. J Clin Monit Comput. 2020. PMID: 31175501 Free PMC article.
-
Cardiac Output Measurement in Neonates and Children Using Noninvasive Electrical Bioimpedance Compared With Standard Methods: A Systematic Review and Meta-Analysis.Crit Care Med. 2022 Jan 1;50(1):126-137. doi: 10.1097/CCM.0000000000005144. Crit Care Med. 2022. PMID: 34325447
Cited by
-
A modified CO-related EIT parameter was used to evaluate pulmonary ventilation-perfusion ratio during prone position and inhaled nitric oxide therapy: a case report.Front Med (Lausanne). 2025 May 26;12:1598248. doi: 10.3389/fmed.2025.1598248. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40491762 Free PMC article.
References
-
- Chew MS, Poelaert J (2003) Accuracy and repeatability of pediatric cardiac output measurement using Doppler: 20-year review of the literature. Intensive Care Med 29:1889–1894 - PubMed
-
- Hsu KH, Wu TW, Wu IH, Lai MY, Hsu SY, Huang HW, Mok TY, Lien R (2017) Electrical cardiometry to monitor cardiac output in preterm infants with patent Ductus Arteriosus: a comparison with echocardiography. Neonatology 112:231–237 - PubMed
-
- Hassan MA, Bryant MB, Hummler HD (2022) Comparison of cardiac output measurement by electrical velocimetry with echocardiography in extremely low birth weight neonates. Neonatology 119:18–25 - PubMed
-
- Song R, Rich W, Kim JH, Finer NN, Katheria AC (2014) The use of electrical cardiometry for continuous cardiac output monitoring in preterm neonates: a validation study. Am J Perinatol 31:1105–1110 - PubMed
-
- Schwarz CE, Livingstone V, O’Toole JM, Healy DB, Panaviene J, Dempsey EM (2022) Agreement of cardiac output estimates between electrical cardiometry and transthoracic echocardiography in very preterm infants. Neonatology 119:594–601 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
