

Impact of sella floor reconstruction on Rathke Cleft Cyst recurrence: a systematic review and meta-analysis
- PMID: 40229623
- PMCID: PMC11996996
- DOI: 10.1007/s11102-025-01521-4
Impact of sella floor reconstruction on Rathke Cleft Cyst recurrence: a systematic review and meta-analysis
Abstract
Background: The optimal surgical technique for managing Rathke's Cleft Cyst (RCC) remains unclear. Leaving the sellar defect open (marsupialisation) after transsphenoidal surgery facilitates ongoing drainage of cyst contents, but cannot be performed in the setting of an intraoperative cerebrospinal fluid (CSF) leak. The effects of intraoperative CSF leaks and sellar floor reconstruction on RCC recurrence require further investigation.
Methods: A systematic literature search was conducted for studies reporting RCC recurrence following transsphenoidal surgery, with data on intraoperative CSF leak rates and skull base reconstruction. Studies were classified based on surgical technique: cyst wall resection vs. fenestration, and open (no reconstruction) vs. closed (reconstructed) sellar floor.
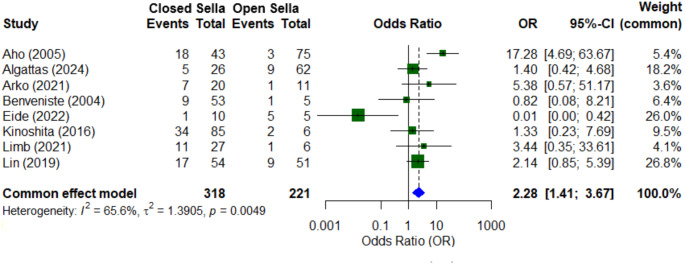
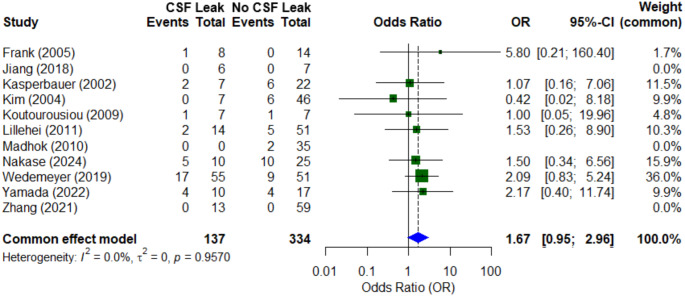
Results: Nineteen studies, comprising 1,076 patients, were included. The overall radiological RCC recurrence rate was 19.8% over a mean follow-up of 50.4 months. The recurrence rate in closed sella surgeries was significantly higher (32.1%) than in open sellar cases (14.0%) (OR 2.28, 95% CI: 1.41-3.67, p < 0.05). Intraoperative CSF leak occurred in 29.1% of cases. Patients with CSF leaks had a higher recurrence rate (23.4% vs. 12.9%), though meta-analysis demonstrated only a non-significant trend (OR 1.67, 95% CI: 0.95-2.96). Subgroup analysis revealed that intraoperative CSF leaks were significantly associated with increased recurrence after fenestration (38.5% vs. 18.4%, p = 0.03), and cyst wall resection (21.7% vs. 7.8%, p = 0.004). In the setting of an intraoperative CSF leak, there was a trend for lower recurrence when cyst wall resection was attempted (21.7% vs. 38.5%, p = 0.09).
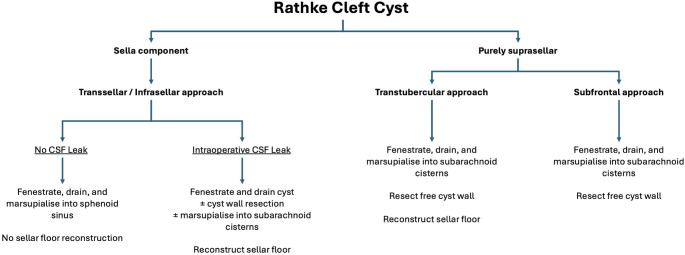
Conclusion: Patients undergoing transsphenoidal surgery for RCC experience high rates of postoperative radiological recurrence. Cyst fenestration while maintaining an open sellar floor (marsupialisation into the sphenoid sinus) is associated with a significantly lower risk of recurrence at over 4 years follow-up. Intraoperative CSF leaks were less strongly associated with cyst recurrence, suggesting that watertight reconstruction, rather than the leak itself, is the primary driver of reaccumulation. When a closed sella is necessitated by intraoperative CSF leak, the addition of cyst wall resection may be associated with a lower rate of recurrence than fenestration alone but must be weighed against a higher risk of AVP-deficiency.
Keywords: Cyst; Flap; Pituitary; Rathke; Reconstruction; Recurrence.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not required. Consent for publication: Not required. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Sphenoid Sinus Mucosal Flap after Transsphenoidal Surgery-A Systematic Review.Medicina (Kaunas). 2024 Feb 6;60(2):282. doi: 10.3390/medicina60020282. Medicina (Kaunas). 2024. PMID: 38399569 Free PMC article.
-
Diaphragm reconstruction using a TachoSil patch as alternative to intrasellar packing for small focal diaphragm defects in pituitary surgery: a cohort study.Acta Neurochir (Wien). 2024 Jun 10;166(1):258. doi: 10.1007/s00701-024-06152-5. Acta Neurochir (Wien). 2024. PMID: 38853198
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Clinical features of Rathke's cleft cyst with secondary hypophysitis and outcomes of endoscopic transnasal surgery versus features of common Rathke's cleft cysts: a single-center retrospective cohort study.J Neurosurg. 2025 Apr 25;143(2):423-430. doi: 10.3171/2025.1.JNS24892. Print 2025 Aug 1. J Neurosurg. 2025. PMID: 40279717
-
Growth dynamics of Rathke's Cleft cyst: a risk score system for surgical decision making.Acta Neurochir (Wien). 2024 Oct 15;166(1):407. doi: 10.1007/s00701-024-06299-1. Acta Neurochir (Wien). 2024. PMID: 39402369 Free PMC article.
Cited by
-
High recurrence of rathke's cleft cysts with anterior-Inferior pituitary displacement despite standard surgical approaches.Pituitary. 2025 Jul 1;28(4):82. doi: 10.1007/s11102-025-01554-9. Pituitary. 2025. PMID: 40593326
References
-
- Trifanescu R, Ansorge O, Wass JAH et al (2012) Rathke’s cleft cysts: Rathke’s cleft cysts. Clin Endocrinol (Oxf) 76:151–160. 10.1111/j.1365-2265.2011.04235.x - PubMed
-
- Castle-Kirszbaum M, Kam J, Wang YY et al (2022) Surgical outcomes and quality of life in Rathke’s cleft cysts undergoing endoscopic transsphenoidal resection: a multicentre study and systematic review of the literature. Pituitary 25:285–295. 10.1007/s11102-021-01197-6 - PubMed
-
- Aho CJ, Liu C, Zelman V et al (2005) Surgical outcomes in 118 patients with Rathke cleft cysts. J Neurosurg 102:189–193. 10.3171/jns.2005.102.2.0189 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
