

Incidence and risk factors of postpartum urinary retention following cesarean section: a retrospective nationwide inpatient sample database study
- PMID: 40229770
- PMCID: PMC11998204
- DOI: 10.1186/s12905-025-03728-w
Incidence and risk factors of postpartum urinary retention following cesarean section: a retrospective nationwide inpatient sample database study
Abstract
Aim: To investigate the risk factors associated with postpartum urinary retention after cesarean section (CS) and to determine the associated morbidity rate.
Methods: This study was a population-based retrospective case-control study analyzed using National Inpatient Sample (NIS) data from 2010 to 2019. The study classified women according to whether they developed postpartum urinary retention after delivery. Predictors of postpartum urinary retention occurring after CS were identified by multivariate logistic regression analysis, and the corresponding incidence rates were examined after adjusting for basic maternal demographic and clinical characteristics.
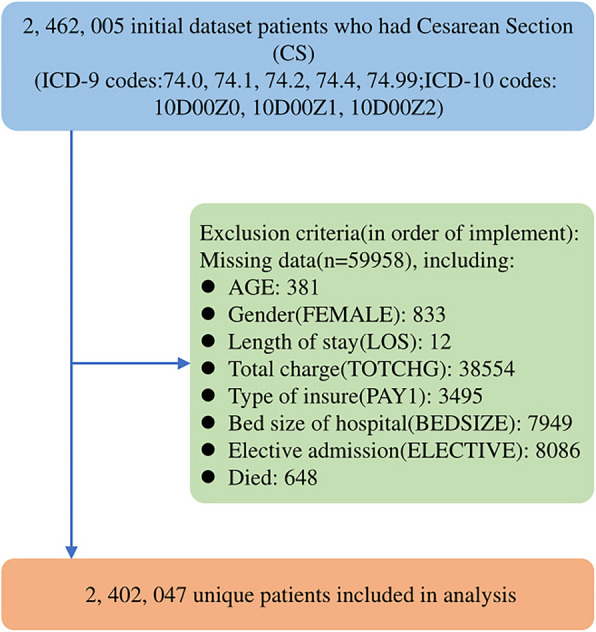
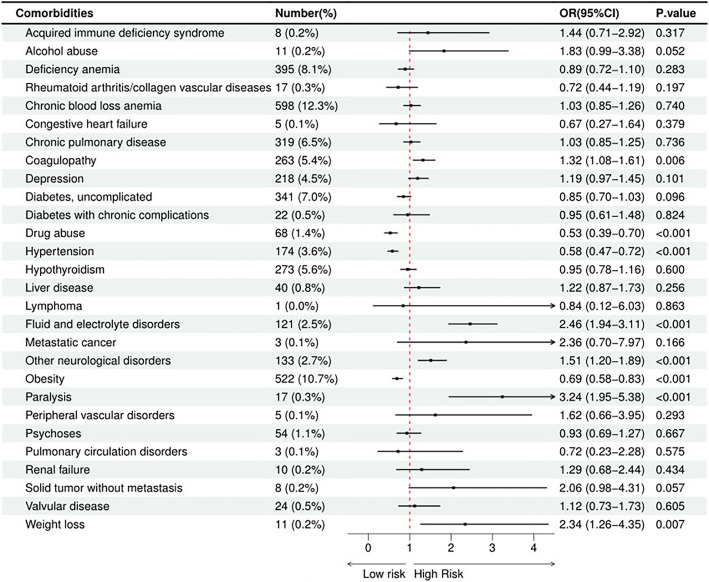
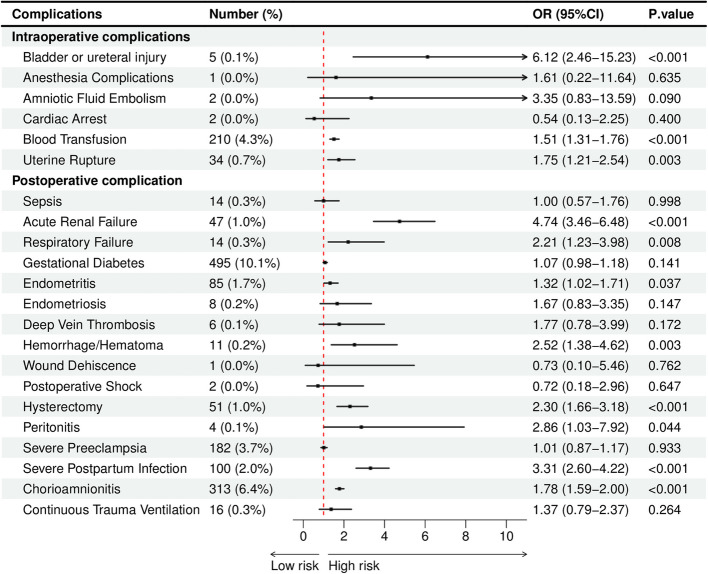
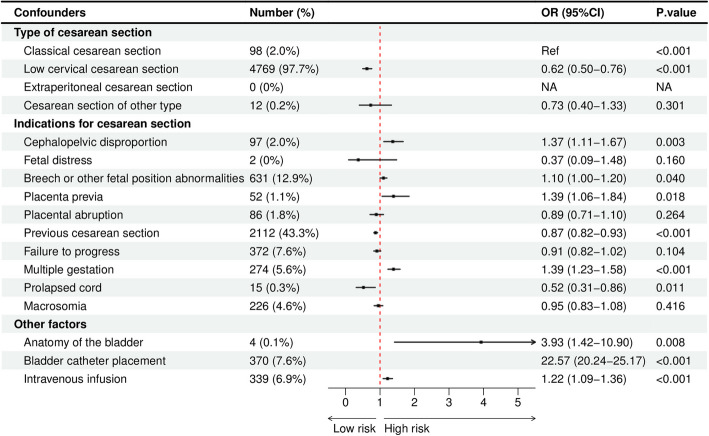
Results: A total of 2,397,168 CSs were extracted from the NIS database. The overall incidence of urinary retention after CS was 0.20%. Patients who experienced urinary retention after CS demonstrated longer length of stay (LOS), higher total costs, and more postoperative complications. The following variables have been identified as potential risk factors for urinary retention: age between 25 and 34 years (OR = 1.27; 95% CI = 1.17-1.38; P < 0.001), 35 years and older (OR = 1.35; 95% CI = 1.22-1.48; P < 0.001), Asian and Pacific Islander (OR = 1.85; 95% CI = 1.68-2.05; P < 0.001), one comorbidity (OR = 1.51; 95% CI = 1.28-1.79; P < 0.001), two comorbidities (OR = 1.51; 95% CI = 1.09-2.08; P = 0.013), three and more comorbidities (OR = 1.79; 95% CI = 1.06-3.04; P = 0.031), large hospitals (OR = 1.16; 95% CI = 1.07-1.26; P < 0.001), teaching hospitals (OR = 1.93; 95% CI = 1.79-2.07; P < 0.001), eastern hospitals (OR = 1.24; 95% CI = 1.14-1.35; P < 0.001), coagulation disorders (OR = 1.32; 95% CI = 1.08-1.61), fluid and electrolyte disorders (OR = 2.46; 95% CI = 1.94-3.11), other neurological disorders (OR = 1.51; 95% CI = 1.20-1.89), paralysis (OR = 3.24; 95% CI = 1.95-5.38), and weight loss (OR = 2.34;95% CI = 1.26-4.35). In addition, urinary retention was associated with postoperative complications related to bladder or ureteral injury (OR = 6.12; 95% CI = 2.46-15.23), blood transfusion (OR = 1.51; 95% CI = 1.31-1.76), acute renal failure (OR = 4.74; 95% CI = 3.46-6.48), respiratory failure (OR = 2.21; 95% CI = 1.23-3.98), endometritis (OR = 1.32; 95% CI = 1.02-1.71), hemorrhage/hematoma ( OR = 2.52; 95% CI = 1.38-4.62), uterine rupture (OR = 1.75; 95% CI = 1.21-2.54), hysterectomy (OR = 2.30; 95% CI = 1.66-3.18), peritonitis (OR = 2.86; 95% CI = 1.03-7.92), severe puerperal infections (OR = 3.31; 95% CI = 2.60- 4.22), chorioamnionitis (OR = 1.78; 95% CI = 1.59-2.00). Notably, the presence of cephalopelvic disproportion (OR = 1.37; 95% CI = 1.11-1.67), breech or other fetal position abnormalities (OR = 1.10; 95% CI = 1.00-1.20), placenta previa (OR = 1.39; 95% CI = 1.06-1.84), multiple gestation (OR = 1.39; 95% CI = 1.23-1.58), anatomy of the bladder (OR = 3.93; 95% CI = 1.42-10.90), bladder catheter placement (OR = 22.57; 95% CI = 20.24-25.17) and intravenous infusion (OR = 1.22; 95% CI = 1.09-1.36) was associated with a significantly increased risk of urinary retention, while low cervical CS (OR = 0.62; 95% CI = 0.50-0.76), previous CS (OR = 0.87; 95% CI = 0.82-0.93) and prolapsed cord (OR = 0.52; 95% CI = 0.31-0.86) conferred some protective effect against it.
Conclusion: In this study, we identified an overall prevalence of 0.20% for urinary retention after CS and several risk factors, including advanced maternal age, Asian and Pacific Islander background, comorbidities, and delivery in large or teaching hospitals, particularly in the Eastern region. Protective factors included hospitals in the southern region, urban hospitals, obesity, and hypertension. Urinary retention was associated with increased postoperative complications, longer LOS, and higher healthcare costs. Several confounders also significantly influenced the incidence of urinary retention. To mitigate these risks, healthcare professionals should prioritize antenatal screening, manage comorbidities, and closely monitor high-risk patients during the postpartum period to reduce adverse outcomes.
Keywords: Cesarean section; National Inpatient Sample; Postpartum urinary retention.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This article does not involve any research on human participants or animals. This observational study used the National Inpatient Sample (NIS) database, a publicly available, research-specific dataset. As is the case with other studies utilizing the NIS, this study did not require ethical review, as the data are anonymised and cannot be linked to any individuals. The NIS dataset has been rigorously desensitised to ensure the security of individual privacy. Researchers use these data solely for statistical analyses or scientific research, with no direct impact on individuals. Therefore, in accordance with relevant ethical review regulations, no consent from individuals is required [78–80]. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- 冯艳丽. Cesarean Delivery Perinatal Complications Management Result Analysis. Advances in Clinical Medicine. 2019;09:711–4.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
