

Diffuse myocardial infiltration in secondary cardiac lymphoma: A case report
- PMID: 40230427
- PMCID: PMC11995691
- DOI: 10.3892/ol.2025.15009
Diffuse myocardial infiltration in secondary cardiac lymphoma: A case report
Abstract
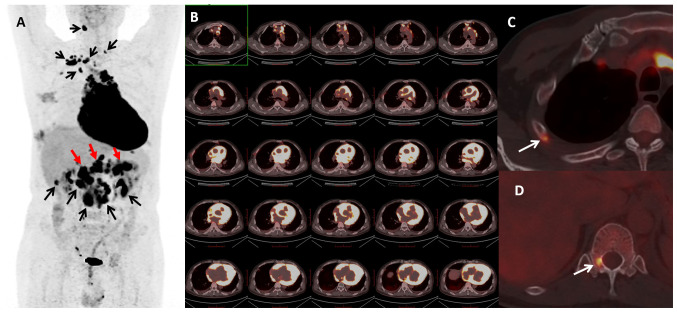
Cardiac lymphomas are rare, with a high proportion developing as secondary lymphomas. The symptoms of secondary heart lymphoma are often nonspecific and may not be detected promptly, leading to a poor prognosis. This case report describes the case of a 53-year-old male patient diagnosed with diffuse large B-cell lymphoma originating in the thymus. Prior to treatment, 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) confirmed the diagnosis of diffuse lymphoma invasion in the heart. After chemotherapy, the cardiac lesions largely regressed. Cardiac magnetic resonance imaging, echocardiography and PET/CT revealed post-chemotherapy tumor necrosis and fibrosis in the myocardium, resulting in the formation of a left ventricular aneurysm. This case report discusses the diagnosis and treatment of secondary cardiac lymphoma, focusing on diffuse myocardial infiltration as the primary manifestation.
Keywords: cardiac lymphoma; case report; diffuse myocardial infiltration; secondary heart lymphoma.
Copyright © 2025, Spandidos Publications.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
A Case of Diffuse Large B-cell Lymphoma with Cardiac Involvement Incidently Diagnosed on Cardiac Imaging.J Coll Physicians Surg Pak. 2021 Sep;31(9):1102-1104. doi: 10.29271/jcpsp.2021.09.1102. J Coll Physicians Surg Pak. 2021. PMID: 34500530
-
Positron emission tomography for the assessment of myocardial viability: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(16):1-80. Epub 2010 Jul 1. Ont Health Technol Assess Ser. 2010. PMID: 23074393 Free PMC article.
-
Distal appendicular skeletal involvement of diffuse large B-cell lymphoma on technetium-99m methylenediphosphonate bone scintigraphy and 18F-fluorodeoxyglucose positron emission tomography/computed tomography: a case report.J Med Case Rep. 2017 Apr 4;11(1):89. doi: 10.1186/s13256-017-1246-y. J Med Case Rep. 2017. PMID: 28372572 Free PMC article.
-
18F-FDG PET/CT in the diagnosis of an extranodal relapse of diffuse large B-cell lymphoma (DLBCL): a clinical case with a literature review.Nucl Med Rev Cent East Eur. 2016;19(B):11-13. doi: 10.5603/NMR.2016.0029. Nucl Med Rev Cent East Eur. 2016. PMID: 27813622 Review.
-
Positron emission tomography/computed tomography in the management of Hodgkin and B-cell non-Hodgkin lymphoma: An update.Cancer. 2021 Oct 15;127(20):3727-3741. doi: 10.1002/cncr.33772. Epub 2021 Jul 19. Cancer. 2021. PMID: 34286864 Review.
Cited by
-
Multisystemic Tuberculosis Masquerading as Aggressive Cardiac Tumor Causing Budd-Chiari Syndrome Disseminated to the Brain Resulting in Death of a Six-Year-Old Boy.Pathogens. 2025 Aug 5;14(8):772. doi: 10.3390/pathogens14080772. Pathogens. 2025. PMID: 40872282 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources