

Preliminary Exploration of Al18F-NOTA-FAPI-04 PET/CT in the Management of Ankylosing Spondylitis: A Prospective Clinical Study
- PMID: 40230596
- PMCID: PMC11995437
- DOI: 10.1177/15353508241270405
Preliminary Exploration of Al18F-NOTA-FAPI-04 PET/CT in the Management of Ankylosing Spondylitis: A Prospective Clinical Study
Abstract
Background: Ankylosing spondylitis (AS) is characterized by inflammation and osteoblastic changes in the sacroiliac joint. As a potential imaging method for the early assessment of AS, positron emission tomography (PET) can quantify systemic disease activity, which is conducive to monitoring the progression of disease activity and assisting in evaluating the efficacy of the treatment.
Objective: The study was to evaluate the diagnostic value of aluminium-[18F]fuoride(Al18F)-labelled fibroblast activation protein inhibitor (FAPI) PET/computed tomography (CT) in AS and to investigate its ability to assess disease activity during the development of AS.
Material and methods: Twenty AS participants who met the Assessment of SpondyloArthritis international Society criteria and were in an active disease stage were included in this study from May 2022 to April 2023. Sixteen healthy controls were also inrolled. All participants underwent Al18F-NOTA-FAPI-04 PET/CT imaging after collecting clinical assessment and laboratory results. The correlation between positive joint count (PJC) and systemic joint standard uptake value ratio (SUVR, the mean SUVmax of the 5 highest joints/SUVmax of the uninvolved sacrum) on PET and clinical disease activity assessment and various laboratory tests were analyzed.
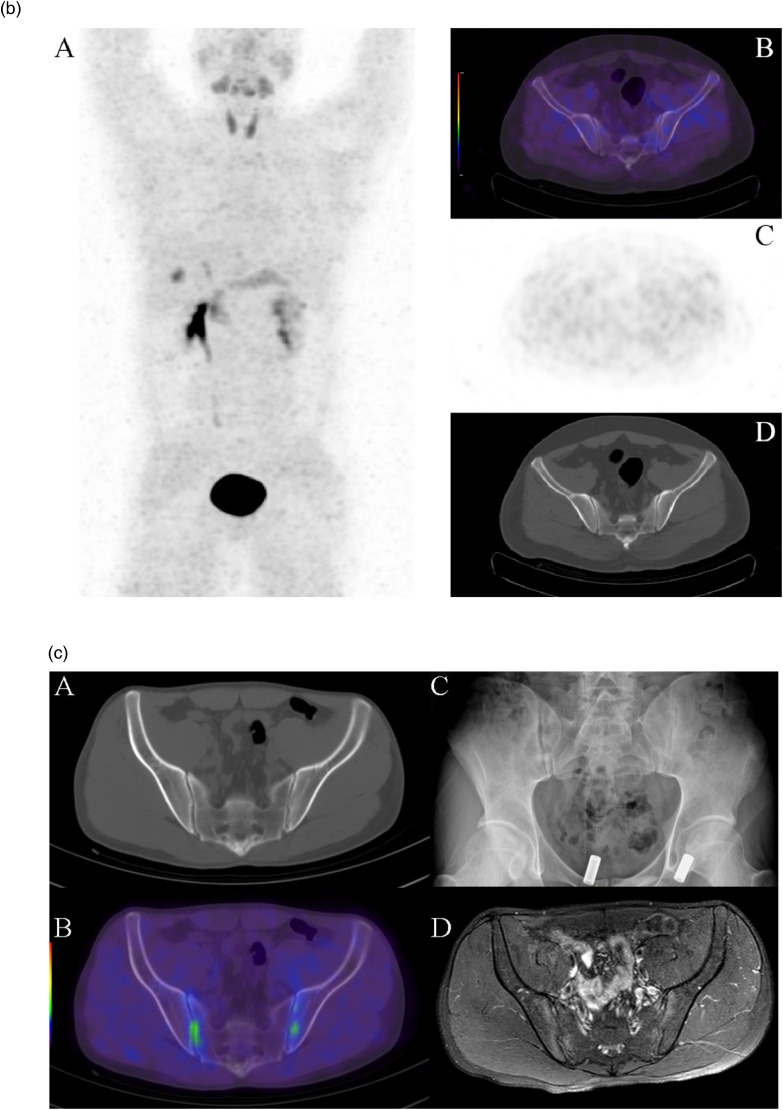
Results: A total of 2820 joints were observed in 20 participants (median age 34.5,[21-61]range, 15 men), with a PJC of 1300 (46.7%), and 39 positive uptakes were found in 40 sacroiliac joints (97.5%). PET/CT images revealed FAPI-04 uptake in both sacroiliac joints in 2 participants without radiographic sacroiliitis in the early stages of AS and varying degrees of uptake in the sacroiliac joints and spinal joints in the remaining participants. PJC and SUVR were positively correlated with most clinical assessments and laboratory findings (P < .05), and SUVR of the sacroiliac joint was positively correlated with C-reactive protein (CRP) (mg/L; r = 0.498, P = .026).
Conclusion: Al18F-NOTA-FAPI-04 PET/CT was highly sensitive to systemic arthritic changes in AS participants and correlated with clinical disease activity and laboratory tests.
Keywords: PET/CT; ankylosing spondylitis; fibroblast activation protein; inflammation.
© The Author(s) 2024.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous