

Breaking the cycle: a comprehensive exploration of topical steroid addiction and withdrawal
- PMID: 40230788
- PMCID: PMC11994697
- DOI: 10.3389/falgy.2025.1547923
Breaking the cycle: a comprehensive exploration of topical steroid addiction and withdrawal
Abstract
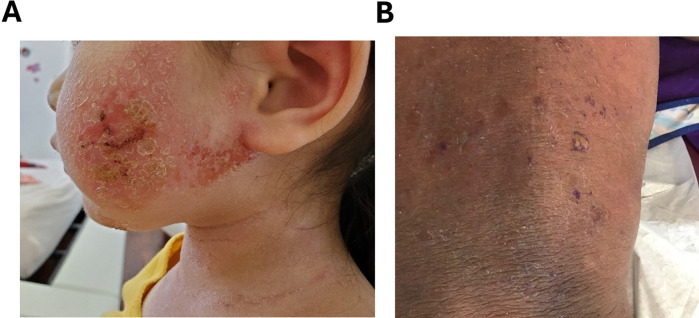
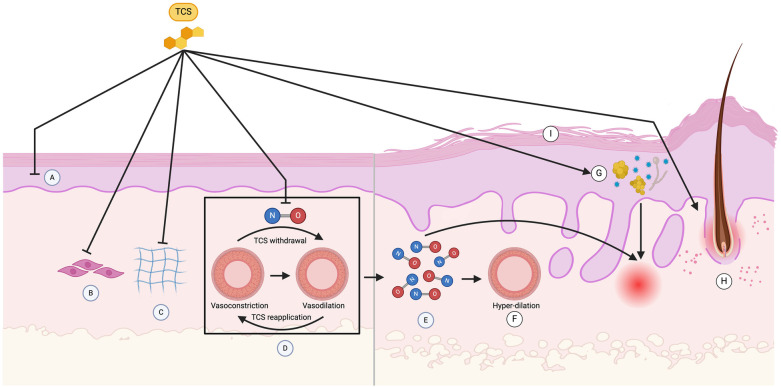
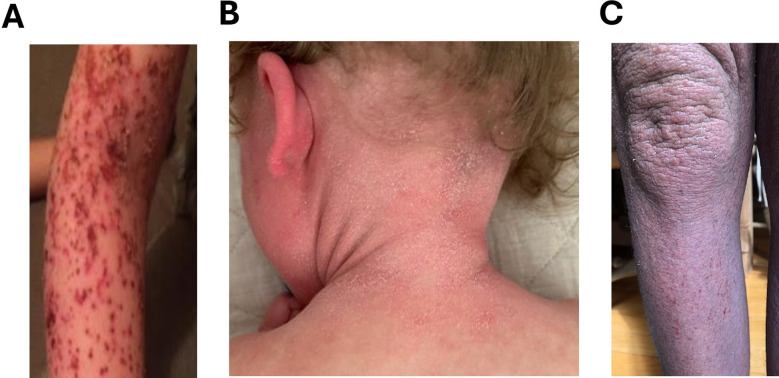
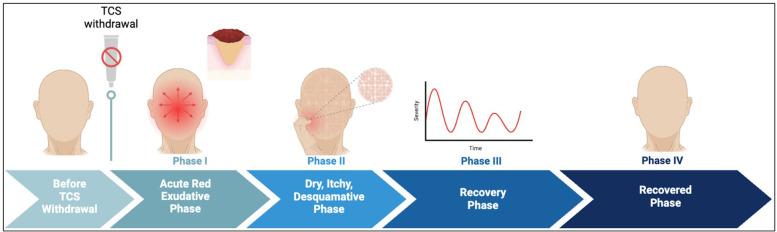
Topical steroid withdrawal (TSW) is a skin condition characterized by red burning, itchy, painful skin lesions, often accompanied by peeling, and cracking. Patients experience sleep disturbances due to intense itching, significantly impacting their quality of life. A majority of affected individuals develop secondary bacterial infection, marked by heavy colonization of Staphylococcus aureus (S. aureus) and alterations in the skin microbiome. TSW is described as a rebound effect following discontinuation of prolonged use of mid-to-high-potency topical corticosteroids. There exist no definitive diagnostic criteria for this entity, and it is often misdiagnosed as a flare-up of an underlying condition or a contact allergy. Despite numerous personal reports and experiences shared on online platforms, studies on TSW remain scarce in scientific literature. Recognizing and effectively managing this condition is critical for healthcare providers seeking to develop comprehensive management plans. These plans typically include supportive therapy for both physical and psychological symptoms, as well as the gradual tapering of corticosteroid use before complete discontinuation. This review aims to consolidate the existing knowledge on TSW, providing a comprehensive resource for its identification, management, and treatment. By enhancing understanding of TSW, this review seeks to support healthcare providers in implementing optimal management strategies and improving patient outcomes.
Keywords: atopic dermatitis; corticosteroids; topical steroid addiction; topical steroid withdrawal; treatment and management.
© 2025 Maskey, Sasaki, Sargen, Kennedy, Tiwari, Geliebter, Safai and Li.
Conflict of interest statement
X-ML receives grants to her institution from the National Institutes of Health, New York State Department of Health/ Empire Clinical Research Investigator Program (ECRIP), the Lie- Artati Family Fund, Study of Integrative Medicine, and Fidelity Charitable DAS Fund; received consultancy fees from FARE, Johnson & Johnson Pharmaceutical Research & Development, L.L.C, Bayer Global Health LLC; received royalties from UpToDate; shares US patent US7820175B2, US10500169B, US10406191B2, US10028985B2, US11351157B2; takes compensation from her practice at the Center for Integrative Health and Acupuncture PC; US Times Technology Inc. is managed by her related party; is a member of General Nutraceutical Technology LLC. AM received partial salary from the Lei-Artati Family fund at New York Medical College. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Sheary B. Topical corticosteroid addiction and withdrawal - an overview for GPs. Aust Fam Physician. (2016) 45(6):386–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources