

Immunotherapeutic strategies in head and neck cancer: challenges and opportunities
- PMID: 40231472
- PMCID: PMC11996880
- DOI: 10.1172/JCI188128
Immunotherapeutic strategies in head and neck cancer: challenges and opportunities
Abstract
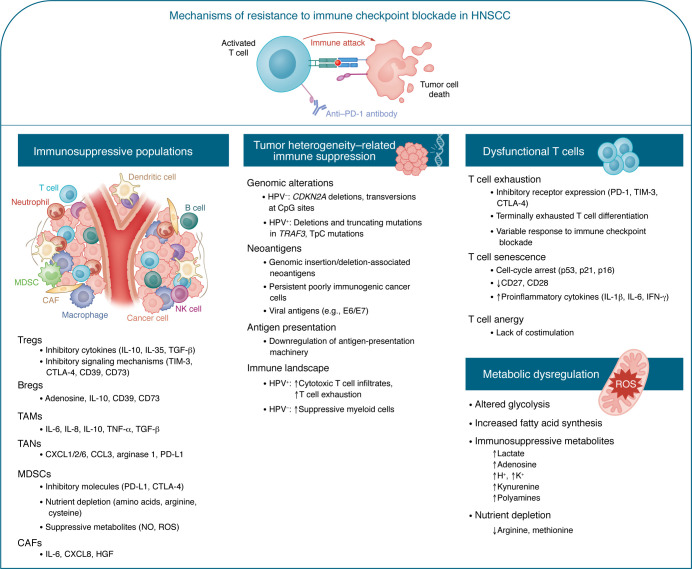
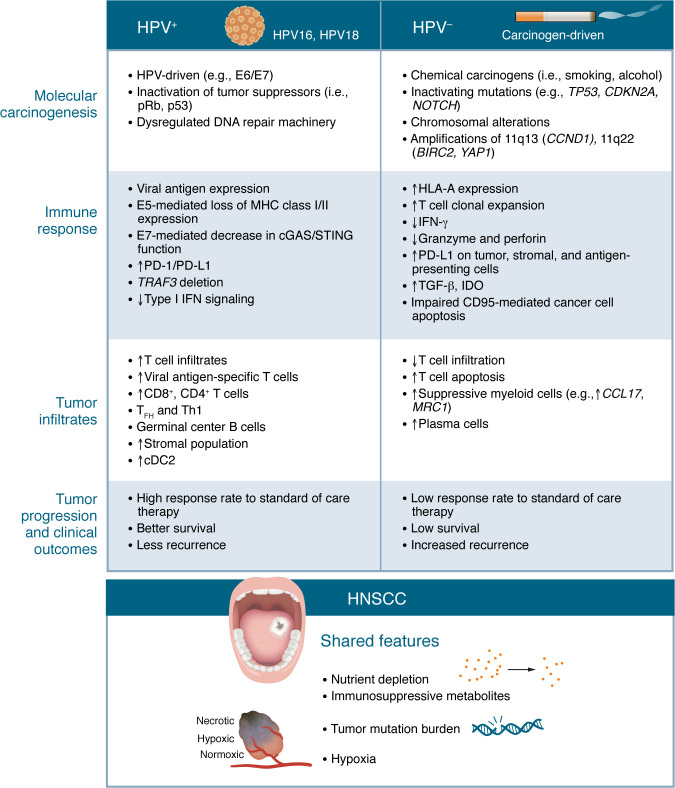
HNSCC remains a substantial health issue, with treatment options including surgery, radiation, and platinum-based chemotherapy. Unfortunately, despite progress in research, only modest gains have been made in disease control, with existing treatments resulting in significant functional and quality-of-life issues. The introduction of immunotherapy in the treatment of HNSCC has resulted in some improvements in outlook for patients and is now standard of care for populations with both recurrent and metastatic disease. However, despite the early successes, responses to immune checkpoint inhibition (ICI) remain modest to low, approaching 14%-22% objective response rates. Challenges to the effectiveness of ICI and other immunotherapies are complex, including the diverse and dynamic molecular plasticity and heterogeneity of HNSCCs; lack of immunogenic antigens; accumulated suppressive immune populations such as myeloid cells and dysfunctional T cells; nutrient depletion; and metabolic dysregulation in the HNSCC tumor microenvironment. In this Review, we explore the mechanisms responsible for immunotherapy resistance, dissect these challenges, and discuss potential opportunities for overcoming hurdles to the development of successful immunotherapy for HNSCC.
Figures

Similar articles
-
Advances and challenges in immunotherapy in head and neck cancer.Front Immunol. 2025 Jun 6;16:1596583. doi: 10.3389/fimmu.2025.1596583. eCollection 2025. Front Immunol. 2025. PMID: 40547025 Free PMC article. Review.
-
Tumor-Specific MHC-II Activates CD4+ and CD8+ T Cells in Head and Neck Squamous Cell Carcinoma to Boost Immunotherapy Efficacy.Cancer Res. 2025 Sep 2;85(17):3258-3274. doi: 10.1158/0008-5472.CAN-24-4383. Cancer Res. 2025. PMID: 40540325 Clinical Trial.
-
Application and Perspectives of Immunotherapy in Head and Neck Squamous Cell Carcinoma.Immunology. 2025 Oct;176(2):164-178. doi: 10.1111/imm.13951. Epub 2025 May 21. Immunology. 2025. PMID: 40396808 Review.
-
Mapping immune activity in HPV-negative head and neck squamous cell carcinoma: a spatial multiomics analysis.J Immunother Cancer. 2025 Jun 25;13(6):e011851. doi: 10.1136/jitc-2025-011851. J Immunother Cancer. 2025. PMID: 40562703 Free PMC article.
-
A systematic review of neoadjuvant and definitive immunotherapy in locally advanced head and neck squamous cell carcinoma.Cancer Med. 2023 May;12(10):11234-11247. doi: 10.1002/cam4.5815. Epub 2023 Mar 19. Cancer Med. 2023. PMID: 36934434 Free PMC article.
Cited by
-
ROS1 mutations promote an immunosuppressive tumor microenvironment via MYC to confer immune evasion in head and neck cancer.Cancer Drug Resist. 2025 Aug 22;8:42. doi: 10.20517/cdr.2025.124. eCollection 2025. Cancer Drug Resist. 2025. PMID: 40873541 Free PMC article.
-
Efficacy and safety of one-time autologous tumor-infiltrating lymphocyte cell therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma.J Immunother Cancer. 2025 Aug 24;13(8):e011633. doi: 10.1136/jitc-2025-011633. J Immunother Cancer. 2025. PMID: 40854613 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
