

The role of gravitational effects and pre-puncture techniques in reducing pneumothorax during CT-guided lung biopsies
- PMID: 40232655
- PMCID: PMC12263723
- DOI: 10.1007/s11547-025-02007-w
The role of gravitational effects and pre-puncture techniques in reducing pneumothorax during CT-guided lung biopsies
Abstract
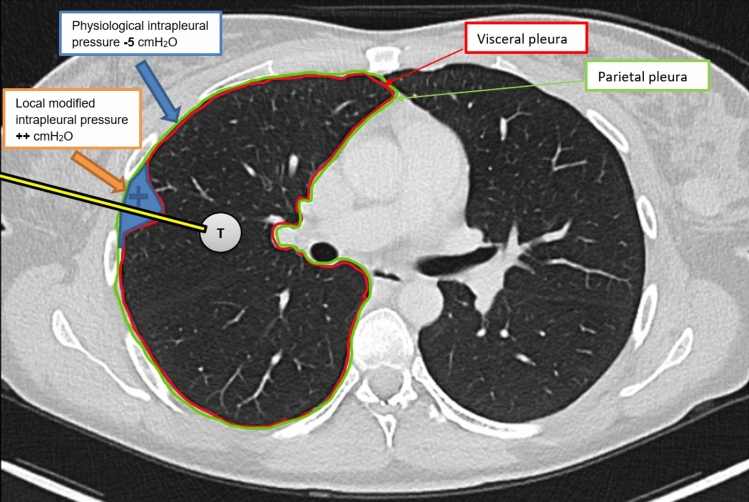
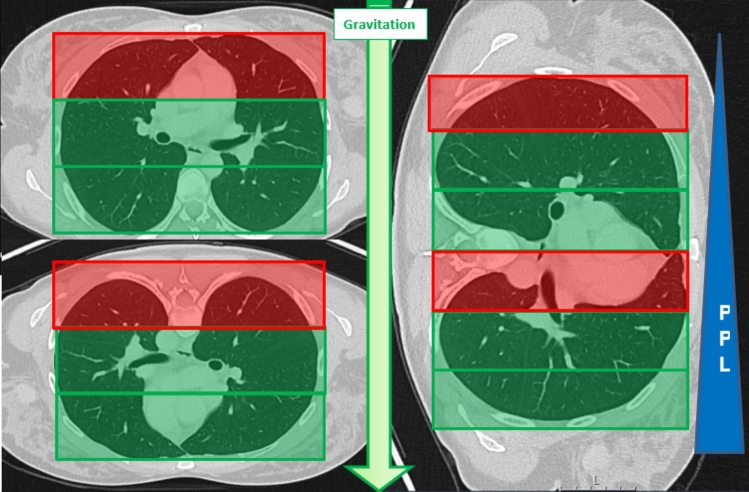
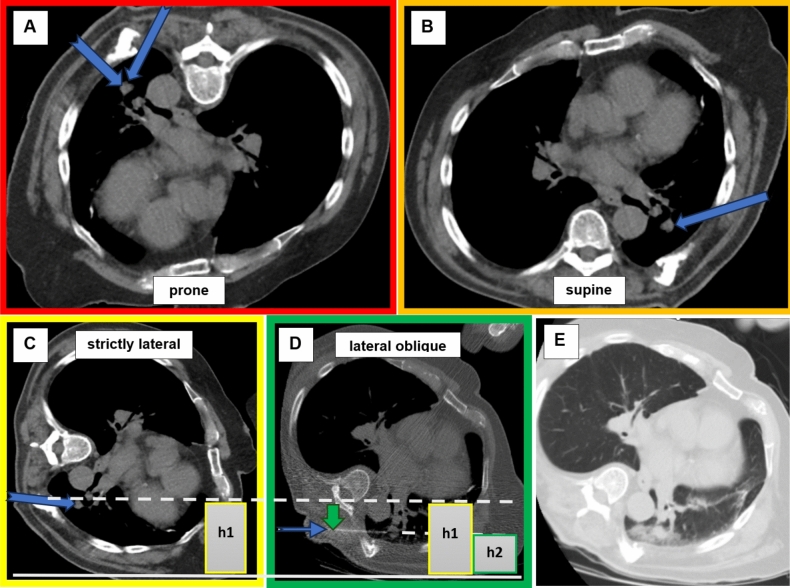
Purpose: The study aimed to evaluate whether the relative height (RH) of the entry point (EP) during CT-guided lung biopsies, adjusted for patient positioning, can predict the risk of pneumothorax during the intervention, leveraging the gravitational effects on pleural pressure.
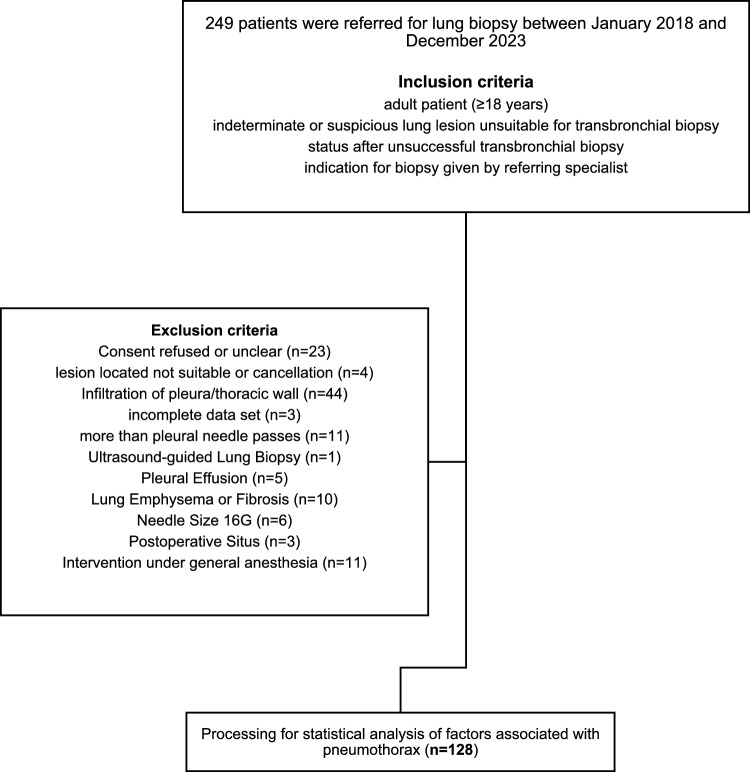
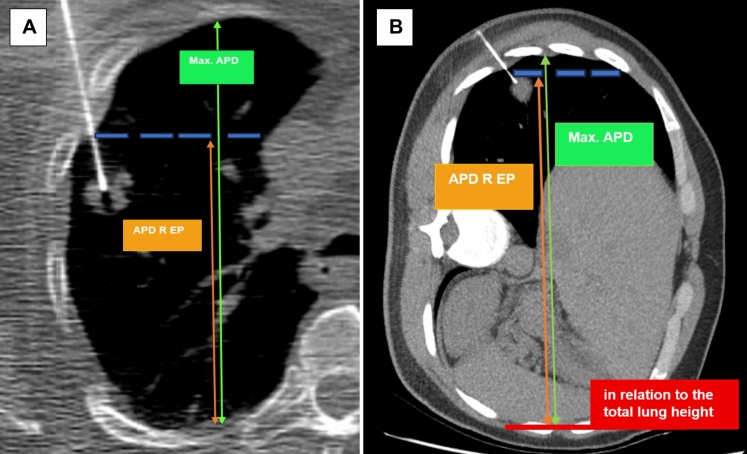
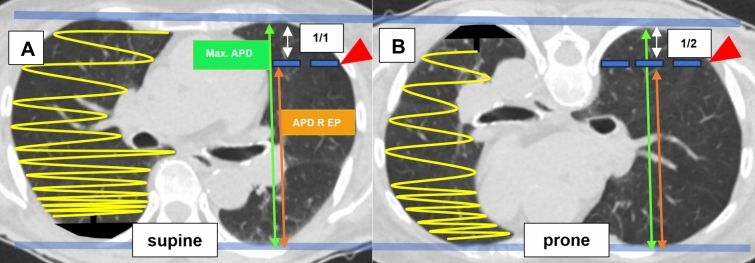
Materials and methods: We retrospectively analyzed 128 percutaneous CT-guided lung biopsies performed at a single center between January 2018 and December 2023. Patients were grouped based on pneumothorax occurrence. Various measurement methods indirectly assessed the influence of gravitational force on pleural pressure, focusing on the RH at the EP with prone positioning adjustments (PP). Other confounding factors like patient demographics, lesion characteristics, pre-puncture fluid administration and other procedural details were assessed. Test performance metrics were compared using Chi-Square, Fisher's exact, and Mann-Whitney U tests. Univariate and binomial logistic regression assessed the influence of different parameters on pneumothorax occurrence.
Results: All measurements of lower RH at EP and pre-puncture fluid administration were significantly associated with a reduced incidence of peri-interventional pneumothorax (p < 0.01). The RH at EP adjusted for the prone position demonstrated the best predictive performance (AUC = 0.844). After adjusting for various confounding factors, both lower RH at EP adjusted for the prone position (OR 110.114, p < 0.001) and pleural fluid administration (OR 0.011, p = 0.011) remained independently associated with a lower risk of pneumothorax.
Conclusion: Strategic use of gravity by selecting the lowest possible entry point, ideally positioning the patient laterally, combined with pre-puncture pleural fluid administration, could be the key to reducing pneumothorax in CT-guided lung biopsies.
Keywords: Biopsy; Image-guided biopsy; Lung; Patient positioning; Pneumothorax; Postoperative complications tomography.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no relevant financial or non-financial interests to disclose. Consent to participate: Informed consent was obtained from all individual participants included in the study. Ethics approval: The study received approval from the Ethics Committee of the Canton of Bern (BASEC ID 2023–00298) and adhered to the principles outlined in the Declaration of Helsinki. The authors had complete access to the data and assumed full responsibility for its integrity.
Figures



Similar articles
-
Pneumothorax risk reduction during CT-guided lung biopsy - Effect of fluid application to the pleura before lung puncture and the gravitational effect of pleural pressure.Eur J Radiol. 2024 Jul;176:111529. doi: 10.1016/j.ejrad.2024.111529. Epub 2024 May 24. Eur J Radiol. 2024. PMID: 38810440
-
Effect of Saline Sealing After CT-Guided Lung Biopsy on Pneumothorax and Hemoptysis.J Comput Assist Tomogr. 2025 Jul-Aug 01;49(4):640-645. doi: 10.1097/RCT.0000000000001725. Epub 2025 Jan 27. J Comput Assist Tomogr. 2025. PMID: 39876517
-
Development and validation of a risk nomogram predicting pneumothorax requiring chest tube placement post-percutaneous CT-guided lung biopsy.BMC Med Imaging. 2025 Jul 1;25(1):220. doi: 10.1186/s12880-025-01794-y. BMC Med Imaging. 2025. PMID: 40597819 Free PMC article.
-
Ultrasound versus computed tomography-guided transthoracic biopsy for pleural and peripheral lung lesions: a systematic review and meta-analysis.Acta Radiol. 2023 Dec;64(12):2999-3008. doi: 10.1177/02841851231206349. Epub 2023 Oct 12. Acta Radiol. 2023. PMID: 37822264
-
Prone position for acute respiratory failure in adults.Cochrane Database Syst Rev. 2015 Nov 13;2015(11):CD008095. doi: 10.1002/14651858.CD008095.pub2. Cochrane Database Syst Rev. 2015. PMID: 26561745 Free PMC article.
Cited by
-
Reevaluating Routine Post-Biopsy Chest X-Rays After CT-Guided Lung Biopsy: Incidence of Pneumothorax and Value of Symptom-Based Monitoring.J Clin Med. 2025 Jul 9;14(14):4867. doi: 10.3390/jcm14144867. J Clin Med. 2025. PMID: 40725566 Free PMC article.
References
-
- Zielinska-Krawczyk M, Krenke R, Grabczak EM, Light RW (2018) Pleural manometry–historical background, rationale for use and methods of measurement. Respir Med 136:21–28 - PubMed
-
- Akulian J, Yarmus L, Feller-Kopman D (2013) The evaluation and clinical application of pleural physiology. Clin Chest Med 34(1):11–19 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
