

Rurality and Area Deprivation and Outcomes After Out-of-Hospital Cardiac Arrest
- PMID: 40232722
- PMCID: PMC12000968
- DOI: 10.1001/jamanetworkopen.2025.3435
Rurality and Area Deprivation and Outcomes After Out-of-Hospital Cardiac Arrest
Abstract
Importance: Large regional variations in outcomes after out-of-hospital cardiac arrest (OHCA) exist.
Objective: To assess whether neighborhood rurality or economic deprivation where an OHCA occurred is associated with variation in emergency medical services (EMS) outcomes after OHCA.
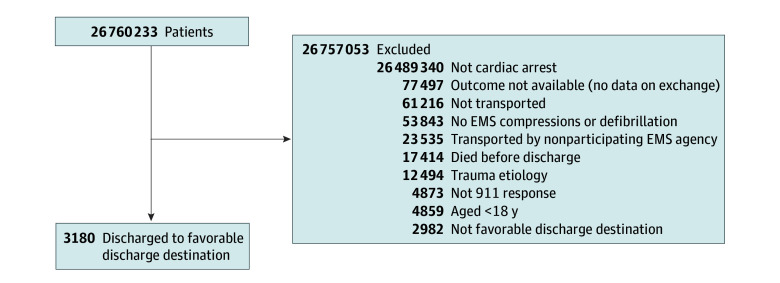
Design, setting, and participants: This cohort study used data collated by ESO Inc on US adult patients (aged ≥18 years) with nontraumatic OHCA receiving chest compressions or defibrillation from EMS between January 1, 2022, and December 31, 2023.
Exposures: Rurality was assessed using Rural-Urban Commuting Area codes. Deprivation was assessed using the Area Deprivation Index. Both were derived from US Census data and grouped by EMS agency.
Main outcomes and measures: Outcomes were restoration of spontaneous circulation (ROSC) at emergency department (ED) arrival, survival to hospital discharge, and favorable discharge destination. Discharge outcomes were only available for patients transported to hospitals using health data exchange. Generalized estimating equations were used to account for correlated data.
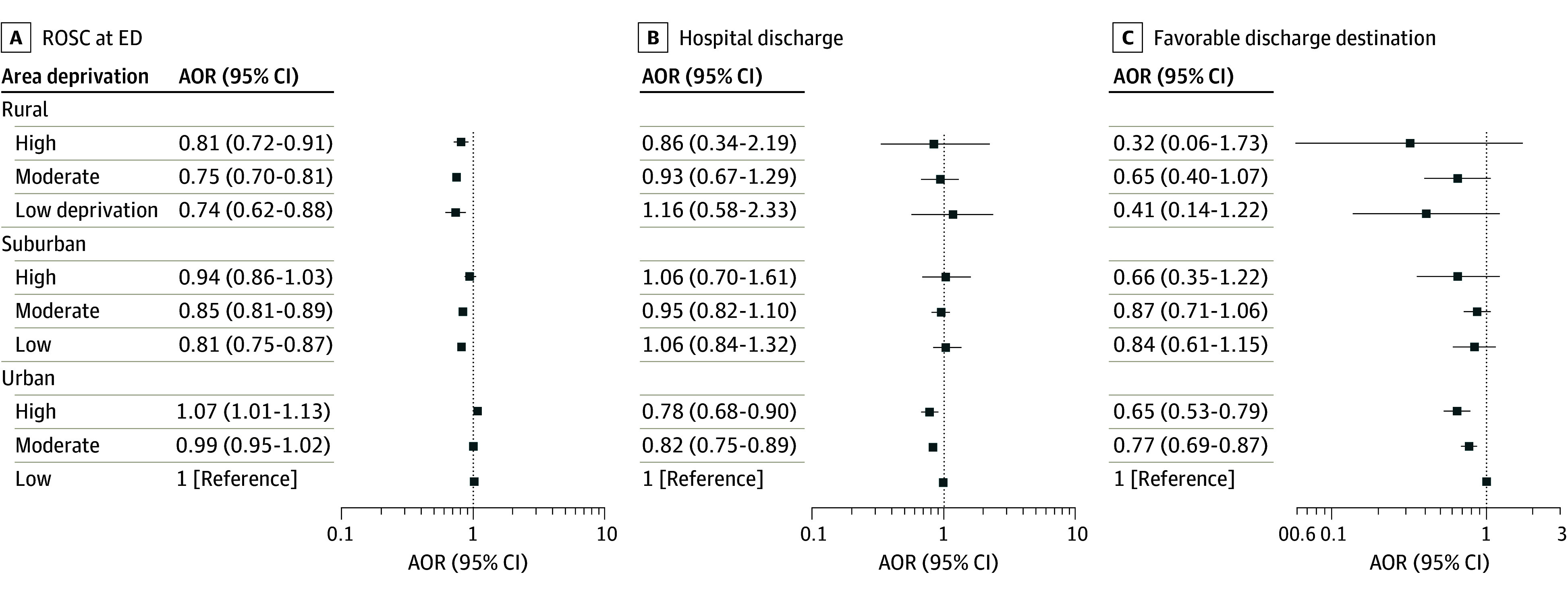
Results: A total of 162 289 patients with OHCA had resuscitation attempted (median [IQR] age, 66 [53-76] years; 62.3% male). Overall, 28.1% of these patients lived in rural or suburban locations, 12.3% lived in areas with high deprivation, 18.7% had a first rhythm of ventricular tachycardia or ventricular fibrillation or shockable by automated external defibrillator rhythm, and 27.6% received bystander cardiopulmonary resuscitation. The mean (SD) EMS response time was 8.7 (5.6) minutes. Upon arrival at the ED, 23.7% of patients had ROSC. Compared with OHCAs in urban areas with low deprivation, those in rural areas with high deprivation (adjusted odds ratio [AOR], 0.81; 95% CI, 0.72-0.91), moderate deprivation (AOR, 0.75; 95% CI, 0.70-0.81), or low deprivation (AOR, 0.74; 95% CI, 0.62-0.88) had lower odds of ROSC at ED arrival. Among patients transported to hospitals using health data exchange, OHCAs in urban areas with high or moderate deprivation had lower odds of survival (AOR, 0.78 [95% CI, 0.68-0.90] and 0.82 [95% CI, 0.75-0.89], respectively) and favorable discharge destination (AOR, 0.65 [95% CI, 0.53-0.79] and 0.77 [95% CI, 0.69-0.87], respectively).
Conclusions and relevance: In this cohort study, OHCAs in rural areas of all levels of economic deprivation were associated with less ROSC at ED arrival vs urban areas with low deprivation, and OHCAs in urban areas with high or moderate deprivation are associated with less survival and less favorable discharge destination, suggesting worse neurologic outcomes. Care improvements alone may not reduce geographic differences in outcomes after OHCA.
Conflict of interest statement
Figures
Similar articles
-
Continuous chest compression versus interrupted chest compression for cardiopulmonary resuscitation of non-asphyxial out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2017 Mar 27;3(3):CD010134. doi: 10.1002/14651858.CD010134.pub2. Cochrane Database Syst Rev. 2017. PMID: 28349529 Free PMC article.
-
Bystander CPR Technique and Outcomes for Cardiac Arrest With and Without Opioid Toxicity.JAMA Netw Open. 2025 Jun 2;8(6):e2516340. doi: 10.1001/jamanetworkopen.2025.16340. JAMA Netw Open. 2025. PMID: 40526383 Free PMC article.
-
Characteristics and outcomes of out-of-hospital cardiac arrest cases responded by emergency medical services across three states in Malaysia.Med J Malaysia. 2025 Mar;80(2):147-152. Med J Malaysia. 2025. PMID: 40145155
-
Gender Differences in Defibrillator Practices in Out-of-Hospital Cardiac Arrest.Prehosp Emerg Care. 2025;29(5):586-592. doi: 10.1080/10903127.2024.2394590. Epub 2024 Sep 17. Prehosp Emerg Care. 2025. PMID: 39189823
-
Cardiopulmonary resuscitation (CPR) plus delayed defibrillation versus immediate defibrillation for out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2014 Sep 12;2014(9):CD009803. doi: 10.1002/14651858.CD009803.pub2. Cochrane Database Syst Rev. 2014. PMID: 25212112 Free PMC article.
References
-
- Blewer AL, McGovern SK, Schmicker RH, et al. ; Resuscitation Outcomes Consortium (ROC) Investigators . Gender disparities among adult recipients of bystander cardiopulmonary resuscitation in the public. Circ Cardiovasc Qual Outcomes. 2018;11(8):e004710. doi:10.1161/CIRCOUTCOMES.118.004710 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
