

Neoadjuvant cobimetinib and atezolizumab with or without vemurafenib for stage III melanoma: outcomes and the impact of the microbiome from the NeoACTIVATE trial
- PMID: 40234093
- PMCID: PMC12001372
- DOI: 10.1136/jitc-2025-011706
Neoadjuvant cobimetinib and atezolizumab with or without vemurafenib for stage III melanoma: outcomes and the impact of the microbiome from the NeoACTIVATE trial
Abstract
Background: Neoadjuvant treatment has become standard for patients with high-risk operable stage III melanoma, but the optimal regimen is unknown. Targeted therapy approaches yield high pathological response rates, while immunotherapy regimens show favorable recurrence-free survival (RFS). NeoACTIVATE was designed to address whether a neoadjuvant combination of both targeted therapy and immunotherapy might leverage the benefits of each.
Methods: We tested neoadjuvant treatment with 12 weeks of vemurafenib, cobimetinib, and atezolizumab for patients with BRAF-mutated (BRAFm) melanoma (cohort A) and cobimetinib and atezolizumab for patients with BRAF-wild-type (BRAFwt) melanoma (cohort B), regimens which we have shown generate a substantial major pathological response. After therapeutic lymph node dissection, patients received 24 weeks of adjuvant atezolizumab. Here, we report survival outcomes and their association with biomarkers assayed among the gut microbiome and peripheral blood immune subsets.
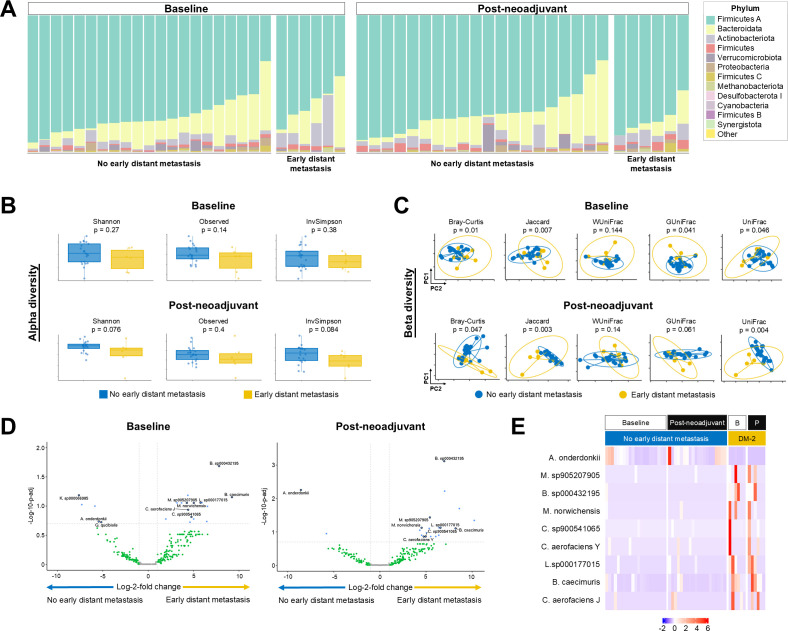
Results: With 49 months median follow-up, the median RFS was not reached for cohort A and was 40.8 months for cohort B. At 24 months after operation, 2 of 14 cohort A patients and 4 of 13 cohort B patients had experienced distant relapse. Key findings from correlative analyses included diversity, taxonomic and functional metagenomic gut microbiome signals associated with distant metastasis-free survival at 2 years. Notably, we observed a strong correlation between low microbial arginine biosynthesis (required for T-cell activation and effector function) and early distant recurrence (p=0.0005), which correlated with taxonomic differential abundance findings. Peripheral blood immune monitoring revealed increased double-positive (CD4+CD8+) T cells in patients with early recurrence.
Conclusions: Neoadjuvant treatment with cobimetinib and atezolizumab±vemurafenib was associated with a low rate of distant metastasis in patients with high-risk stage III melanoma. Freedom from early distant metastasis was highly associated with taxonomic differences in gut microbiome structure and with functional pathway alterations known to modulate T cell immunity. Identification of predictive biomarkers will permit optimization of neoadjuvant therapy regimens for individual patients.
Trial registration number: NCT03554083.
Keywords: Immune Checkpoint Inhibitor; Immunotherapy; Neoadjuvant; Skin Cancer; Surgery.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: MSB: Research support—Alkermes, Bristol-Myers Squibb, Genentech, Merck, nFerence, Perspective Therapeutics, Pharmacyclics, Regeneron, Sorrento, TILT Biotherapeutics, and Transgene; Consultant/Scientific Advisory Board—Perspective Therapeutics, Sorrento Therapeutics, TILT Biotherapeutics; RRM: Research support—Glaxo SmithKline and Bristol-Myers Squibb; LAK: Consultant/Scientific Advisory Board—Immunocore; SNM: Research support—Bristol-Myers Squibb; Royalties—Sorrento Therapeutics and Journey Therapeutics; AD: Research support—Syntrix Pharmaceuticals, Novartis, Merck, AnHearth Therapeutics, Sorrento Therapeutics, Guardant, Philogen, AstraZeneca; Consultant/Scientific Advisory Board—TP Therapeutics, Guardant Health, AnHeart Therapeutics, Chromacode; Honoraria—Intellisphere; MAP: Research support—Intuitive Surgical; DLP: Consultant/Scientific Advisory Board—In Situ Biologics; TJH: Research support—Genentech and SkylineDX BV.
Figures




References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials