

Clinical effects of combination therapy with continuous renal replacement therapy and continuous intravenous sodium infusion therapy
- PMID: 40234097
- PMCID: PMC12213318
- DOI: 10.1111/1744-9987.70021
Clinical effects of combination therapy with continuous renal replacement therapy and continuous intravenous sodium infusion therapy
Abstract
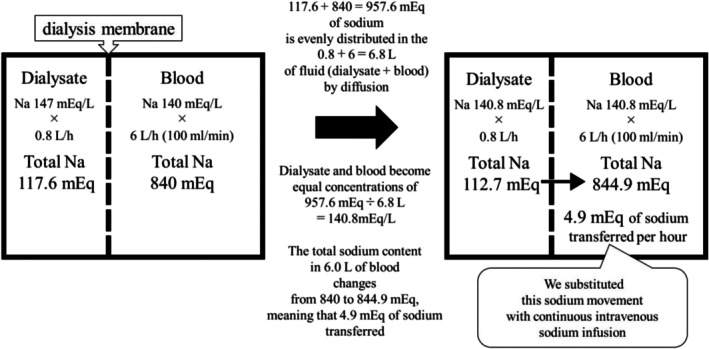
Introduction: This single-center retrospective study investigated the clinical effects of combination therapy involving continuous renal replacement therapy (CRRT) and continuous intravenous sodium infusion therapy (cIVNa) in critically ill patients with prerenal acute kidney injury (AKI) who were expected to experience insufficient plasma refilling.
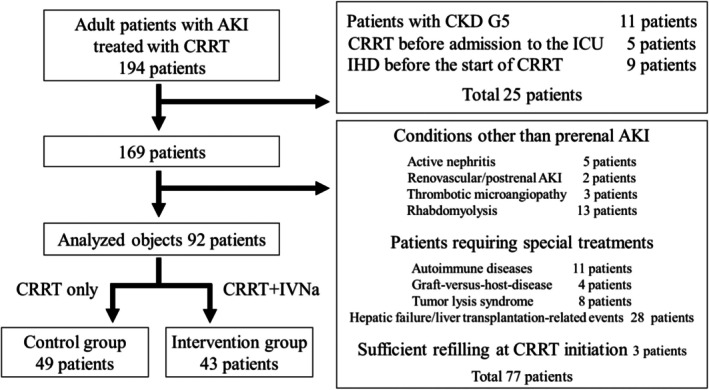
Method: The clinical data of 92 patients were analyzed. Clinical data from the control (CRRT, n = 49) and intervention (CRRT + cIVNa, n = 43) groups were compared statistically.
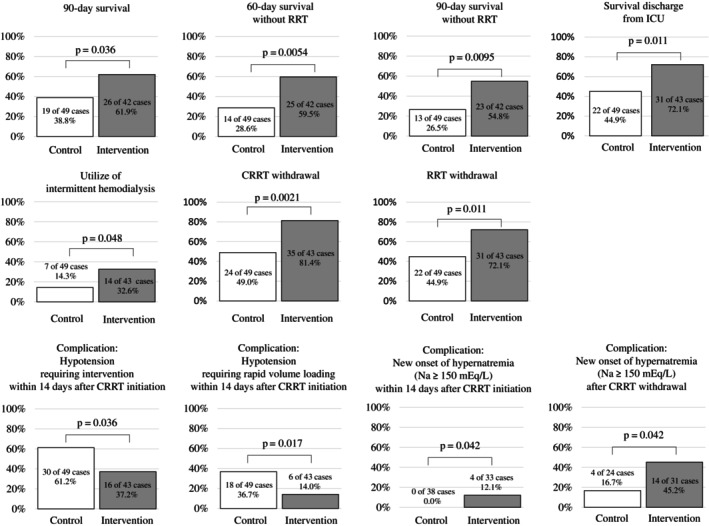
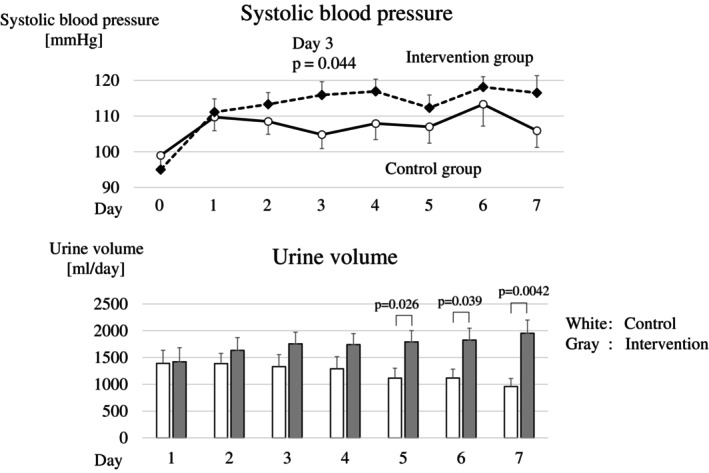
Results: Combination therapy increased blood pressure and urine volume, while reducing hypotension events, indicating hemodynamic stabilization. Furthermore, it significantly improved the 90-day survival rate (61.9% vs. 38.8%, p < 0.05), 60-day and 90-day survival rates without RRT (59.5% vs. 28.6%, p < 0.01; 54.8% vs. 26.5%, p < 0.01, respectively), survival discharge rate from intensive care unit, CRRT withdrawal rate, and renal replacement therapy withdrawal rate.
Conclusion: Combination therapy with continuous renal replacement therapy and continuous intravenous sodium infusion therapy may be a useful treatment option for critically ill patients with prerenal acute kidney injury who require continuous renal replacement therapy.
Keywords: acute kidney injury; continuous renal replacement therapy; high‐sodium dialysate; multimodal approach; plasma refilling.
© 2025 The Author(s). Therapeutic Apheresis and Dialysis published by John Wiley & Sons Australia, Ltd on behalf of International Society for Apheresis and Japanese Society for Apheresis.
Conflict of interest statement
The authors declare that they have no conflicts of interest or competing interests.
Figures
Similar articles
-
Reduction Rate of Uric Acid in Blood during Continuous Renal Replacement Therapy for Acute Kidney Injury: A Multicenter Retrospective Observational Study.Blood Purif. 2025;54(2):83-92. doi: 10.1159/000542329. Epub 2024 Oct 29. Blood Purif. 2025. PMID: 39471783 Free PMC article.
-
Intensity of continuous renal replacement therapy for acute kidney injury.Cochrane Database Syst Rev. 2016 Oct 4;10(10):CD010613. doi: 10.1002/14651858.CD010613.pub2. Cochrane Database Syst Rev. 2016. PMID: 27699760 Free PMC article.
-
Outcomes of renal replacement therapy in acute kidney injury: factors associated with dialysis dependence and progression to end-stage renal disease - a MarketScan database analysis.Ren Fail. 2025 Dec;47(1):2504015. doi: 10.1080/0886022X.2025.2504015. Epub 2025 May 21. Ren Fail. 2025. PMID: 40400240 Free PMC article.
-
Determinants of Urine Output Using Advanced Hemodynamic Monitoring in Critically Ill Patients Undergoing Continuous Renal Replacement Therapy.Blood Purif. 2024;53(3):189-199. doi: 10.1159/000535544. Epub 2023 Dec 16. Blood Purif. 2024. PMID: 38104538
-
Interventions to prevent hemodynamic instability during renal replacement therapy in critically ill patients: a systematic review.Crit Care. 2018 Feb 22;22(1):41. doi: 10.1186/s13054-018-1965-5. Crit Care. 2018. PMID: 29467008 Free PMC article.
References
-
- Vinsonneau C, Camus C, Combes A, Costa de Beauregard MA, Klouche K, Boulain T, et al. Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple‐organ dysfunction syndrome: a multicentre randomised trial. Lancet. 2006;368(9533):379–385. - PubMed
-
- Lins RL, Elseviers MM, Van der Niepen P, Hoste E, Malbrain ML, Damas P, et al. Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: results of a randomized clinical trial. Nephrol Dial Transplant. 2009;24(2):512–518. 10.1093/ndt/gfn560 - DOI - PubMed
-
- Bellomo R, Cass A, Cole L, Finfer S, Gallagher M, Lo S, et al. Intensity of continuous renal‐replacement therapy in critically ill patients. N Engl J Med. 2009;361(17):1627–1638. - PubMed
-
- Gaudry S, Hajage D, Schortgen F, Martin‐Lefevre L, Pons B, Boulet E, et al. Initiation strategies for renal‐replacement therapy in the intensive care unit. N Engl J Med. 2016;375(2):122–133. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
