

Deep insight into cytokine storm: from pathogenesis to treatment
- PMID: 40234407
- PMCID: PMC12000524
- DOI: 10.1038/s41392-025-02178-y
Deep insight into cytokine storm: from pathogenesis to treatment
Abstract
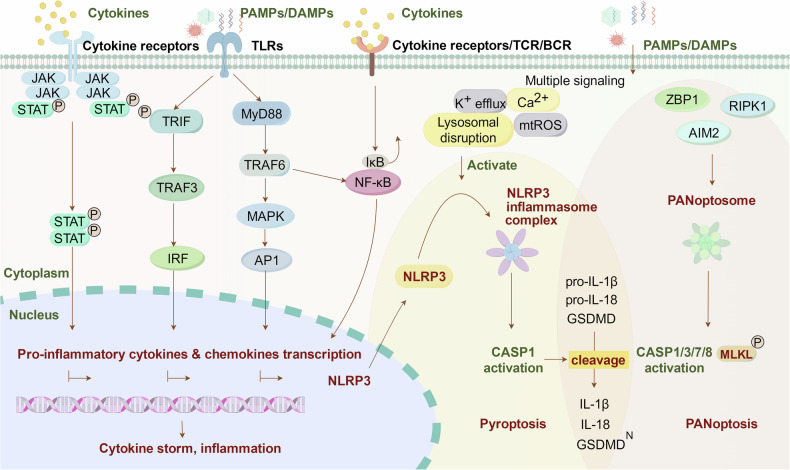
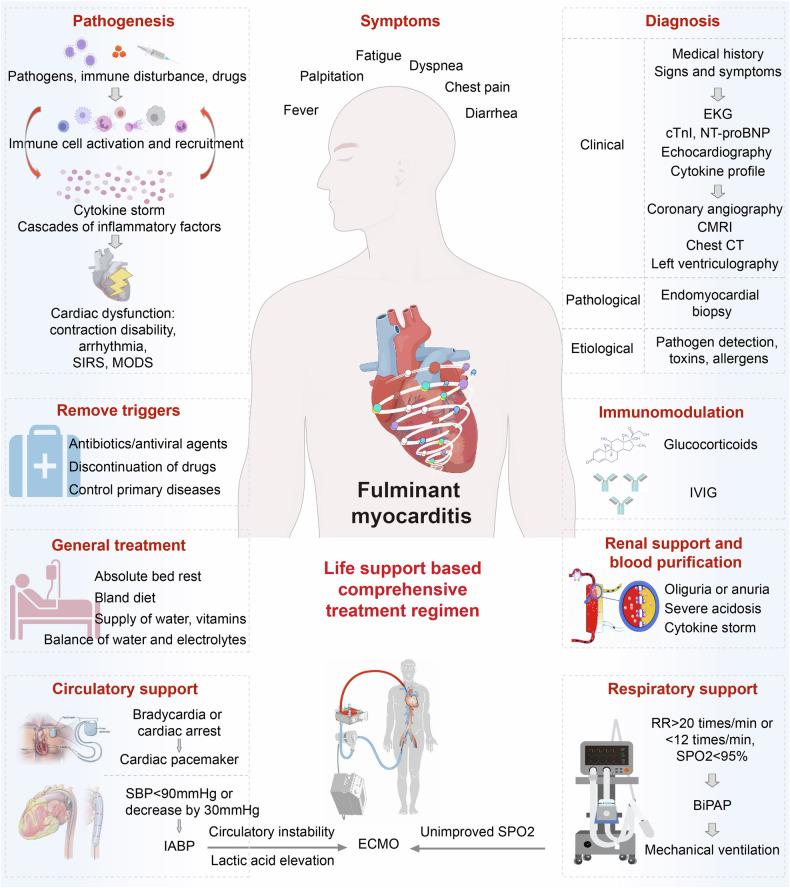
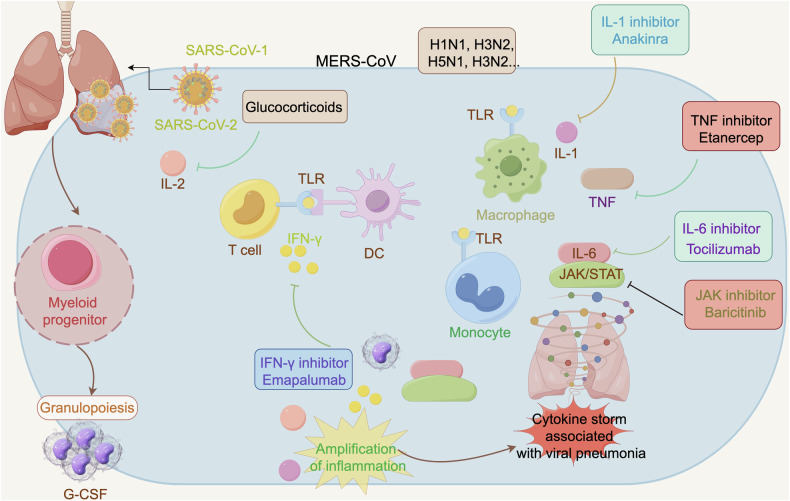
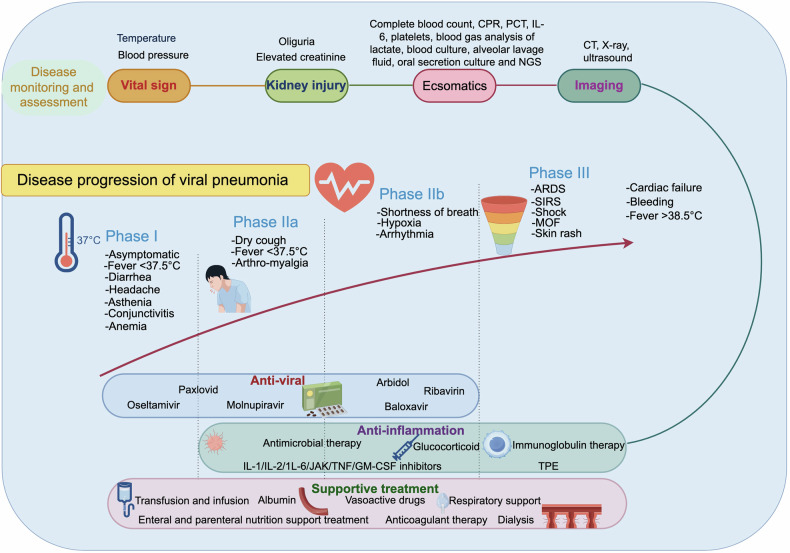
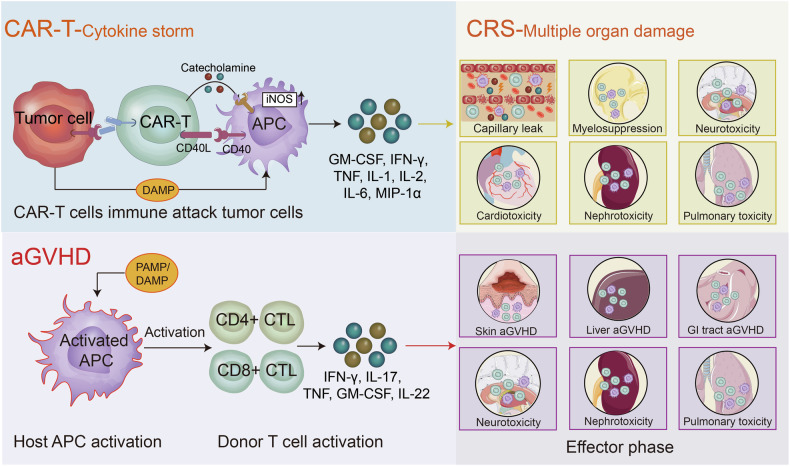
Cytokine storm (CS) is a severe systemic inflammatory syndrome characterized by the excessive activation of immune cells and a significant increase in circulating levels of cytokines. This pathological process is implicated in the development of life-threatening conditions such as fulminant myocarditis (FM), acute respiratory distress syndrome (ARDS), primary or secondary hemophagocytic lymphohistiocytosis (HLH), cytokine release syndrome (CRS) associated with chimeric antigen receptor-modified T (CAR-T) therapy, and grade III to IV acute graft-versus-host disease following allogeneic hematopoietic stem cell transplantation. The significant involvement of the JAK-STAT pathway, Toll-like receptors, neutrophil extracellular traps, NLRP3 inflammasome, and other signaling pathways has been recognized in the pathogenesis of CS. Therapies targeting these pathways have been developed or are currently being investigated. While novel drugs have demonstrated promising therapeutic efficacy in mitigating CS, the overall mortality rate of CS resulting from underlying diseases remains high. In the clinical setting, the management of CS typically necessitates a multidisciplinary team strategy encompassing the removal of abnormal inflammatory or immune system activation, the preservation of vital organ function, the treatment of the underlying disease, and the provision of life supportive therapy. This review provides a comprehensive overview of the key signaling pathways and associated cytokines implicated in CS, elucidates the impact of dysregulated immune cell activation, and delineates the resultant organ injury associated with CS. In addition, we offer insights and current literature on the management of CS in cases of FM, ARDS, systemic inflammatory response syndrome, treatment-induced CRS, HLH, and other related conditions.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: D.W.W. is the editorial board member of Signal Transduction and Targeted Therapy, but he has not been involved in the process of the manuscript handling. The authors declare no competing interests.
Figures



References
-
- Flemming, A. Sleep deprivation whips up cytokine storm. Nat. Rev. Immunol.24, 2 (2024). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 82070217, 81873427/National Natural Science Foundation of China (National Science Foundation of China)
- 82100401/National Natural Science Foundation of China (National Science Foundation of China)
- 81772477, 81201848, 82473220/National Natural Science Foundation of China (National Science Foundation of China)
- 82330010,81630010,81790624/National Natural Science Foundation of China (National Science Foundation of China)
LinkOut - more resources
Full Text Sources
