

Biomarker and cognitive decline in atrial fibrillation: a prospective cohort study
- PMID: 40234472
- PMCID: PMC12000550
- DOI: 10.1038/s41598-025-89800-9
Biomarker and cognitive decline in atrial fibrillation: a prospective cohort study
Abstract
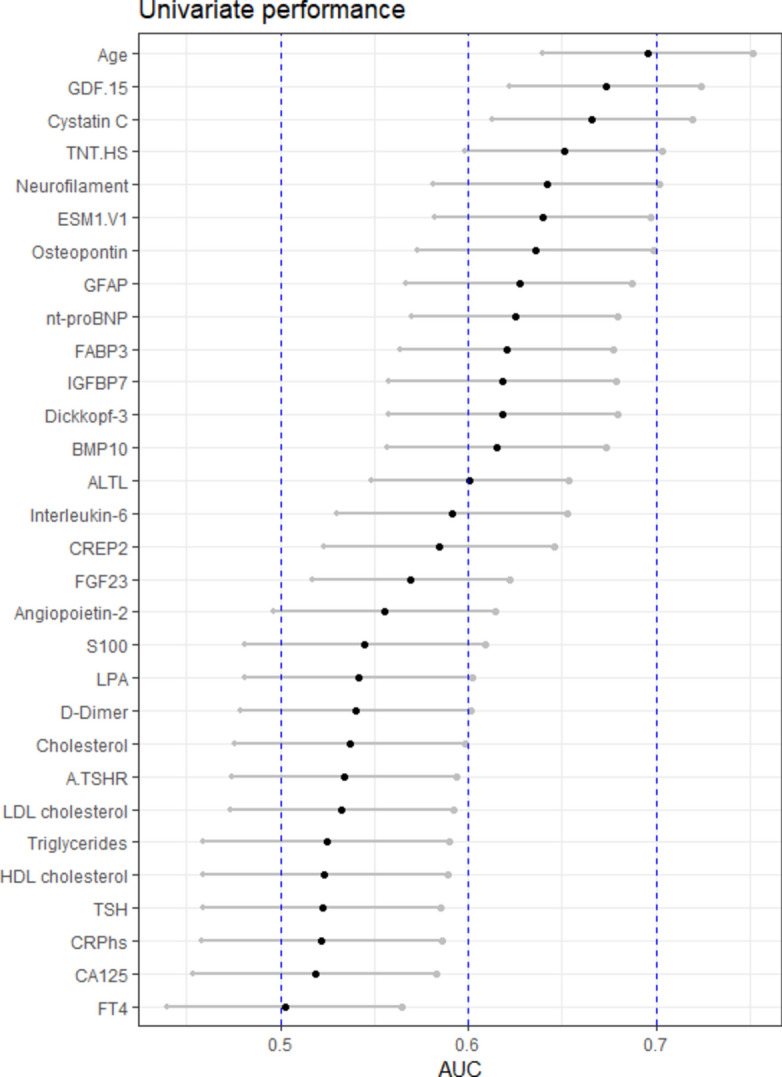
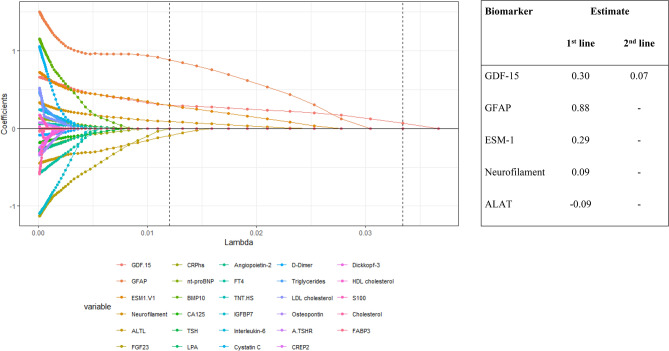
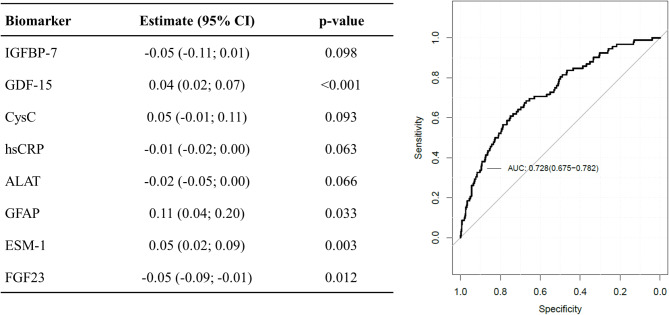
We investigated associations of a broad biomarker panel with cognitive decline in atrial fibrillation (AF) patients to characterize possible mechanisms. We enrolled 1440 AF patients with available baseline biomarkers and cognitive testing by the Montreal Cognitive assessment (MoCA) score at inclusion and at ≥ 2 yearly follow-ups. We investigated the associations of biomarkers with cognitive decline in univariate logistic regression models, LASSO regression analysis and built a combined model. Mean age was 72 years, 75% male, 47% paroxysmal AF. Over 4 years, 93 patients (6.5%) had cognitive decline. These patients had more often permanent AF (32.3 vs 21.5%, p = 0.007) and more often a history stroke (23.7 vs 11.2%, p < 0.001), but similar baseline MoCA scores (24.9 vs 25.3 points, p = 0.22) and anticoagulation rates (93.5 vs 89.5%, p = 0.29). The three biomarkers with the highest univariate AUC for cognitive decline were GDF-15 (0.67 [0.62-0.72]), Cystatin C (0.67 [0.61-0.72]) and high-sensitivity Troponin T (hs-TnT) (0.65 [0.60-0.70]). In LASSO regression analysis, the best cross validation included GDF-15, GFAP, ESM-1, NfL and ALAT. The combined prediction model with the highest AUC of 0.73 (0.68-0.78) included IGFBP-7, GDF-15, Cystatin C, hsCRP, ALAT, GFAP, ESM-1 and FGF23. Over 4 years, 6.5% of AF patients had cognitive decline despite a high rate of anticoagulation. Inflammation, neuronal damage, and increased amyloid-beta might be important non-ischemic mechanisms of cognitive decline in AF patients.
Keywords: Atrial fibrillation; Biomarker; Cognitive decline.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Andreas S. Müller received fellowship and training support from Biotronik, Boston Scientific, Medtronic, Abbott/St. Jude Medical, and Biosense Webster. Speaker honoraria from Biosense Webster, Medtronic, Abbott/St. Jude Medical, AstraZeneca, Daiichi Sankyo, Biotronik, MicroPort, Novartis. Consultant for Biosense Webster, Medtronic, Abbott/St. Jude Medcal, and Biotronik (all outside of the current work). David Conen received consulting fees from Roche Diagnostics, and speaker fees from Servier and BMS/Pfizer, all outside of the current work. Giorgio Moschovitis received advisory board or speaker’s fees from Astra Zeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Gebro Pharma, Novartis and Vifor, all outside of the submitted work. Jürg H. Beer reports grant support from the Swiss National Foundation of Science, The Swiss Heart Foundation and the Stiftung Kardio; grant support, speakers- and consultation fees to the institution from Bayer, Sanofi and Daichii Sankyo. Leo H. Bonati reports personal fees and nonfinancial support from Amgen, grants from AstraZeneca, personal fees and nonfinancial support from Bayer, personal fees from Bristol-Myers Squibb, personal fees from Claret Medical, grants from Swiss National Science Foundation, grants from University of Basel, grants from Swiss Heart Foundation, outside the submitted work. Michael Kühne reports grants from Bayer, grants from BMS, grants from Boston Scientific, grants from Daiichi Sankyo, grants from Pfizer, personal fees from Abbott, personal fees from Boston Scientific, personal fees from Daiichi Sankyo. Philipp Krisai reports speaker fees from BMS/Pfizer and research grants from the Swiss National Science Foundation, Swiss Heart Foundation, Foundation for Cardiovascular Research Basel, Machaon Foundation. Richard Kobza receives institutional grants from Abbott, Biosense-Webster, Boston-Scientific, Biotronik, Medtronic and Sis-Medical. Stefan Osswald Research grant from Swiss National Science Foundation (SNSF) for Swiss AF Cohort study (33CS30_18474/1&2). Research grant from Swiss National Science Foundation (SNSF) for Swiss AF Control study (324730_192394/1). Research grants from Swiss Heart Foundation (SHS). Research grants from Foundation for CardioVascular Research Basel (SKFB). Research grants from Roche. Educational and Speaker Office grants from Roche, Bayer, Novartis, Sanofi AstraZeneca, Daiichi-Sankyo, Pfizer. Tobias Reichlin has received research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union [Eurostars 9799 – ALVALE), and the Cardiovascular Research Foundation Basel, all for work outside the submitted study. He has received speaker/consulting honoraria or travel support from Abbott/SJM, Astra Zeneca, Brahms, Bayer, Biosense-Webster, Biotronik, Boston-Scientific, Daiichi Sankyo, Medtronic, Pfizer-BMS, and Roche, all for work outside the submitted study. He has received support for his institution’s fellowship program from Abbott/SJM, Biosense-Webster, Biotronik, Boston-Scientific, and Medtronic, for work outside the submitted study. Stefanie Aeschbacher received speaker fee from Roche Diagnostics.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
