

Multicenter retrospective cohort study of the sequential use of the antibody-drug conjugates (ADCs) trastuzumab deruxtecan (T-DXd) and sacituzumab govitecan (SG) in patients with HER2-low metastatic breast cancer (MBC)
- PMID: 40234477
- PMCID: PMC12000457
- DOI: 10.1038/s41523-025-00748-5
Multicenter retrospective cohort study of the sequential use of the antibody-drug conjugates (ADCs) trastuzumab deruxtecan (T-DXd) and sacituzumab govitecan (SG) in patients with HER2-low metastatic breast cancer (MBC)
Abstract
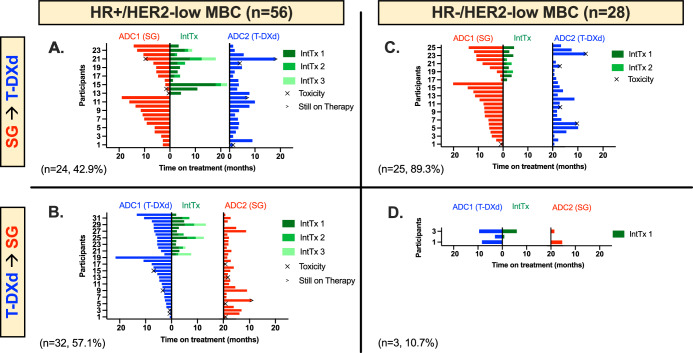
Antibody drug conjugates (ADCs) have improved outcomes for patients with metastatic breast cancer (MBC), but there is little data about the sequential use of these agents. In this multicenter retrospective cohort study, we identified 84 patients with HER2-low MBC treated sequentially with trastuzumab deruxtecan (T-DXd) and sacituzumab govitecan (SG) in either order at 5 institutions between 2020-2024. We evaluated clinical parameters associated with time to treatment failure (TTF) and real-world overall survival (rwOS). Median TTF was longer for ADC1 than ADC2, irrespective of HR-status, ADC sequence order, age ≤65 or >65 years, presence of visceral disease, or use of an intervening therapy. Younger age, longer time from MBC diagnosis to start of ADC1, and receipt of SG as ADC1 were associated with longer rwOS from start of ADC1. This cohort represents one of the first multicenter retrospective series of patients treated with sequential ADCs for HER2-low MBC, which may inform clinical practice.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: LAH: AdBoard: Pfizer, AstraZeneca. Research funding to institution: Greenwich LifeSciences. Book royalties: McGraw Hill. RM: Consultant/advisor: Agendia, Arvinas, Astra Zeneca, Daiichi, Eisai, Genentech, Gilead, Hologic, Lilly, Novartis, Pfizer, Puma, Sanofi, Sermonix, Stemline. Research support (paid to institution): Gilead. SF: No disclosures. ND: Consulting: Gilead, Novartis, Lilly, Pfizer, MJH Life Sciences, PrecisCa, Neogenomics. SP: No disclosures. AR: Employment at Bristol Myers Squibb. SJ: No disclosures. LQ: No disclosures. MM: For Myself: Research funding to institution: Pfizer, KCRN Research, Puma, OBI Pharma. For spouse: Speaker bureau/honoraria: Gilead, Astra Zeneca/Daichi-sankyo; Stock Ownership: Merrimack. JC: Research funding to institution: Merck, Puma, Amgen, Seagen, Pfizer, Olema. Ad board: Genentech. AS: Adboard: Merck, AstraZenca, Stemline, Genzyme, Gilead. LC: AdBoard/consulting: AstraZeneca/Daiichi Sankyo. MA: Consulting: Bayer, Xoft, Apollomics, Viewray, Cairn Therapeutics, AnheartTherapeutics, Theraguix, MenariniRicerche, Sumitomo Pharma Oncology, Autem therapeutics, GT Medical Technologies, Allovir, EquilliumBio., QV Bioelectronics, Servier Pharmaceuticals, Incyte. DSMC: VBI Vaccines Scientific Advisory Board: Modifibiosciences., Bugworks Shareholder: Mimivax, Cytodyn, MedInnovateAdvisors LLC, TrisalusLifesciences Funding: 1R01CA277728-01A1, 1R01 CA264017-01A1. NH: No disclosures. JH: AdBoard/consulting: AstraZeneca. AB: No COI relevent to this paper. KB: No disclosures. MK: No disclosures. DI: No disclosures. RR: Consulting/Advisory Boards: AstraZeneca, DSI, Ter-sera, Lilly, Genentech, Lilly, Pfizer, Merck. KG: Advisory board with honoraria to institution for Astra Zeneca, Novartis, Puma Biotechnologies, Eli Lilly, Gilead, Exact Sciences, Neogenomics and Tersera Therapeutics. HR: Institutional research support: AstraZeneca; Daiichi Sankyo, Inc.; F. Hoffmann-La Roche AG/Genentech, Inc.; Gilead Sciences, Inc.; Lilly; Merck & Co., Inc.; Novartis Pharmaceuticals Corporation; Pfizer; Stemline Therapeutics, OBI Pharma; Ambryx. Consultancy/advisory: Chugai, Puma, Napo.
Figures
References
-
- Bardia, A. et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med.384, 1529–1541 (2021). - PubMed
-
- Rugo, H. S. Overall survival (OS) results from the phase III TROPiCS-02 study of sacituzumab govitecan (SG) vs treatment of physician’s choice (TPC) in patients (pts) with HR+/HER2- metastatic breast cancer (mBC). Presented at: ESMO; September 9, 2022; Paris, France.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
