

Evaluation of a two-tier preterm birth prevention service in a tertiary hospital in the United Kingdom: a retrospective cohort study
- PMID: 40234805
- PMCID: PMC11998394
- DOI: 10.1186/s12884-025-07538-8
Evaluation of a two-tier preterm birth prevention service in a tertiary hospital in the United Kingdom: a retrospective cohort study
Abstract
Background: Preterm birth is the most important cause of neonatal morbidity and mortality. Clinical guidelines recommend assessment of risk of preterm birth and implementation of interventions to reduce preterm birth risk through dedicated preterm birth clinics. We hypothesized that a two-tier preterm birth clinic pathway can safely manage women at the highest risk of preterm birth while reducing intervention for women at moderate risk of preterm birth. We aimed to test this hypothesis by evaluating risk factors, management, and outcomes of women attending a two-tier preterm birth prevention service.
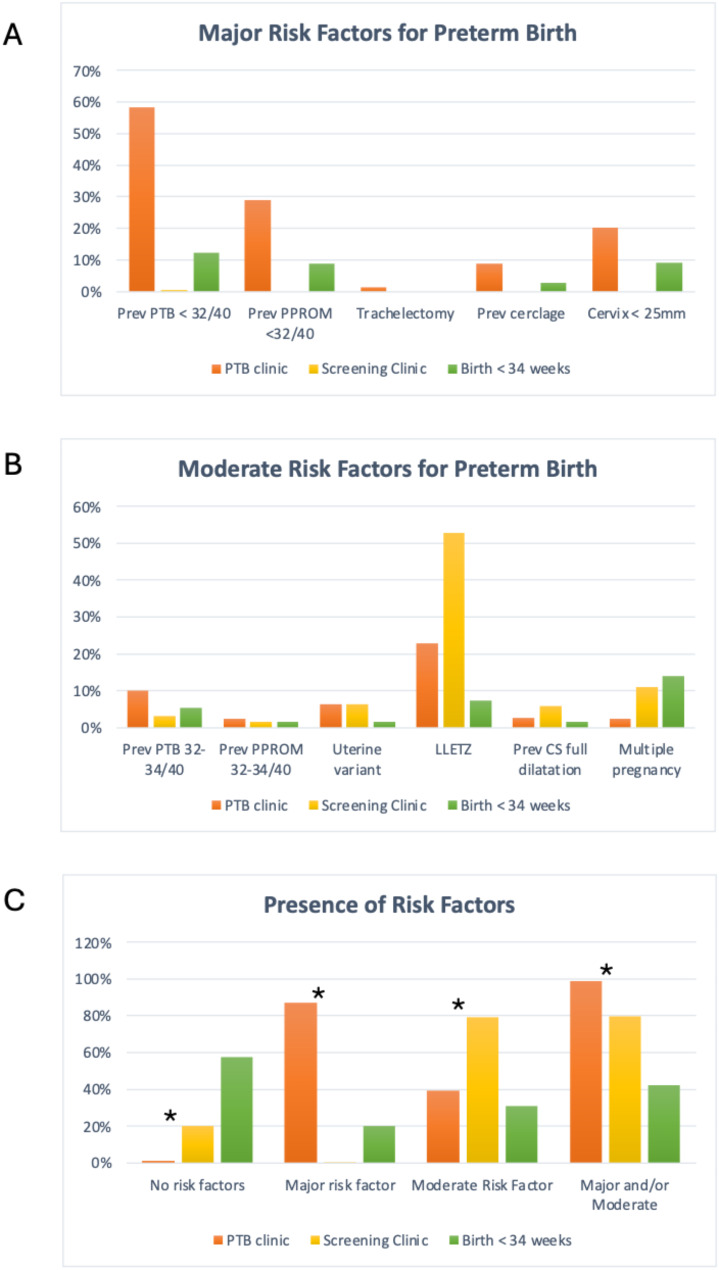
Methods: We conducted a retrospective cohort study of women who gave birth between January and June 2021 at a tertiary hospital in Oxford, UK. We included two cohorts: women attending a Cervical Screening Clinic and women attending a Preterm Birth Clinic, and we also reviewed all cases of births before 34 weeks over that time period. At the initial midwife appointment at 8-10 weeks' gestation, risk factors for preterm birth were assessed. Pregnant women with moderate risk factors (previous preterm birth at 32+ 0 - 33+ 6 weeks, previous preterm prelabour rupture of membranes (PPROM) at 32+ 0 - 33+ 6 weeks, previous LLETZ / cone biopsy, known abnormal uterus, previous caesarean section at 10 cm dilatation, and multiple pregnancy) were referred to the Cervical Screening Clinic for a cervical length scan by a sonographer. Pregnant women with major risk factors (previous preterm birth at 16+ 0 - 31+ 6 weeks, previous PPROM at less than 32+ 0 weeks, radical trachelectomy, previous cervical cerclage) as well as those with a cervix < 25 mm at any scan were referred to the Preterm Birth Clinic for a cervical length scan and counselling by a specialist obstetrician. Detailed information on risk factors, management, and perinatal outcomes were collected from case notes and analysed.
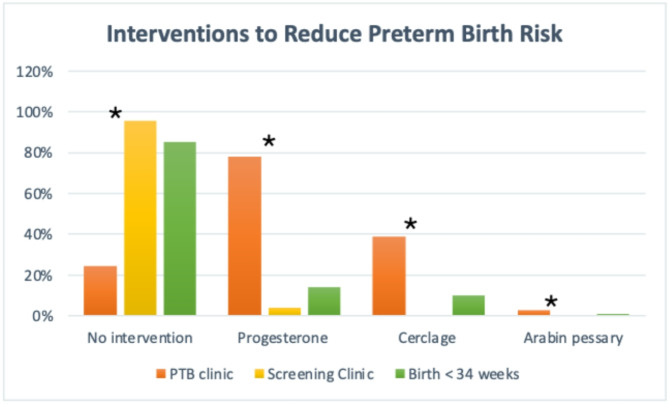
Results: 189 women attended the Cervical Screening Clinic: 79.1% had a moderate risk factor for preterm birth, 100% had a cervical length scan, 7% had a short cervix and 4.2% received an intervention. All 196 infants were live born, with overall preterm birth rates of 14.8% at < 37 weeks, 3.1% at < 32 weeks, and 0% at < 28 weeks. The spontaneous live preterm birth rates were 9.7% at < 37 weeks, 2.6% at < 32 weeks and 0% at < 28 weeks. 79 women attended the Preterm Birth Clinic: 87.3% had a major risk factor for preterm birth, 100% had ≥ 1 cervical length scan, 41.3% had a short cervix, 78.1% received vaginal progesterone, and 39% had a cervical cerclage. Overall preterm birth rates were 33.8% at < 37 weeks, 10.3% at < 32 weeks and 4.4% at < 28 weeks. Spontaneous live preterm birth rates were 22.1% at < 37 weeks, 7.4% at < 32 weeks, and 2.9% at < 28 weeks. 115 women gave birth to 130 babies before 34 weeks: 80% had no major risk factor for preterm birth, 29% had a cervical length scan and less than 15% had an intervention. Over 90% had a live birth, but the neonatal death rate was high (8.5%).
Conclusion: Women with moderate risk factors for preterm birth seen in the Cervical Screening Clinic had low rates of intervention and good perinatal outcomes. Most women with major risk factors were appropriately referred and managed by the Preterm Birth Clinic. This two-tier preterm birth prevention service therefore appears safe and effective.
Keywords: Cervical cerclage; Cervical length; Preterm birth; Progesterone; Risk factor; Ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed as part of a service evaluation using routinely collected data. The study was registered with the Oxford University Hospitals NHS Foundation Trust audit department. The study was reviewed by the Joint Research Office of Oxford University Hospitals NHS Foundation Trust and Oxford University, and was deemed not to need formal ethical approval as it falls under the category of a service evaluation study. This is in line with the guidance from the United Kingdom NHS Health Research Authority ( https://www.hra.nhs.uk/approvals-amendments/what-approvals-do-i-need/ ) stating that explicit consent for use of patient information for clinical audit and service improvement purposes is not required. Consent for publication: Not Applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Efficacy of ultrasound-indicated cerclage in twin pregnancies: a retrospective case-control study matched by cervical length.Am J Obstet Gynecol MFM. 2023 Mar;5(3):100847. doi: 10.1016/j.ajogmf.2022.100847. Epub 2023 Jan 11. Am J Obstet Gynecol MFM. 2023. PMID: 36638868
-
Utility of follow-up cervical length screening in low-risk women with a cervical length of 26 to 29 mm.Am J Obstet Gynecol. 2021 Aug;225(2):179.e1-179.e6. doi: 10.1016/j.ajog.2021.02.027. Epub 2021 Feb 27. Am J Obstet Gynecol. 2021. PMID: 33652056 Free PMC article.
-
"Does the use of gestation-specific centiles for cervical length change the management of pregnancies at risk of recurrent spontaneous preterm birth?".Eur J Obstet Gynecol Reprod Biol. 2021 Sep;264:349-352. doi: 10.1016/j.ejogrb.2021.07.052. Epub 2021 Jul 31. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 34385081
-
Cervical stitch (cerclage) in combination with other treatments for preventing spontaneous preterm birth in singleton pregnancies.Cochrane Database Syst Rev. 2020 Sep 24;9(9):CD012871. doi: 10.1002/14651858.CD012871.pub2. Cochrane Database Syst Rev. 2020. PMID: 32970845 Free PMC article.
-
[Prevention of spontaneous preterm birth (excluding preterm premature rupture of membranes): Guidelines for clinical practice - Text of the Guidelines (short text)].J Gynecol Obstet Biol Reprod (Paris). 2016 Dec;45(10):1446-1456. doi: 10.1016/j.jgyn.2016.09.011. Epub 2016 Nov 9. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 27836377 Review. French.
References
-
- National Institute of Health and Care Excellence. Preterm labour and birth NICE guideline [NG25]. 2015. Available from: www.nice.org.uk/guidance/ng25 - PubMed
-
- NHS England. Saving babies’ lives: version 3. A care bundle for reducing perinatal mortality. 2023. Available from: https://www.england.nhs.uk/long-read/saving-babies-lives-version-3/
-
- UK Preterm Clinical Network. Reducing Preterm Birth: Guidelines for Commissioners and Providers. 2019. https://www.tommys.org/sites/default/files/2021-03/reducing preterm birt...
-
- Ferrero DM, Larson J, Jacobsson B, Renzo GC, Di, Norman JE, Martin JN et al. Cross-Country individual participant analysis of 4.1 million Singleton births in 5 countries with very high human development index confirms known associations but provides no biologic explanation for 2/3 of all preterm births. PLoS ONE. 2016;11(9):e0162506. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
