

Sex-specific trunk movement coordination in participants with low-back pain and asymptomatic controls
- PMID: 40235462
- PMCID: PMC11996882
- DOI: 10.3389/fspor.2025.1524489
Sex-specific trunk movement coordination in participants with low-back pain and asymptomatic controls
Abstract
Background: Trunk posture and lumbo-pelvic coordination can influence spinal loading and are commonly used as clinical measures in the diagnosis and management of low-back pain and injury risk. However, sex and pain specific characteristics have rarely been investigated in a large cohort of both healthy individuals and low-back pain patients. It has also been suggested that the motor control of trunk stability and trunk movement variability is altered in individuals with low-back pain, with possible implications for pain progression. Nonetheless, clear links to low-back pain are currently lacking.
Objective: To investigate trunk posture, lumbo-pelvic coordination, trunk dynamic stability and trunk movement variability in an adequately large cohort of individuals with low-back pain and asymptomatic controls and to explore specific effects of sex, pain intensity and pain chronicity.
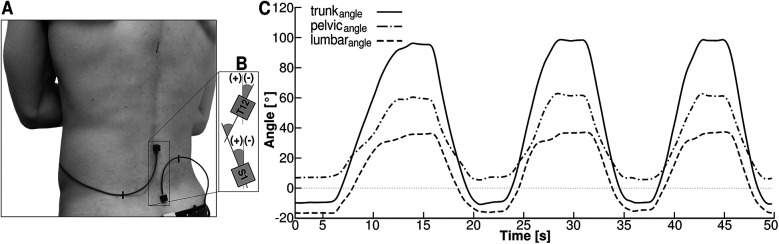
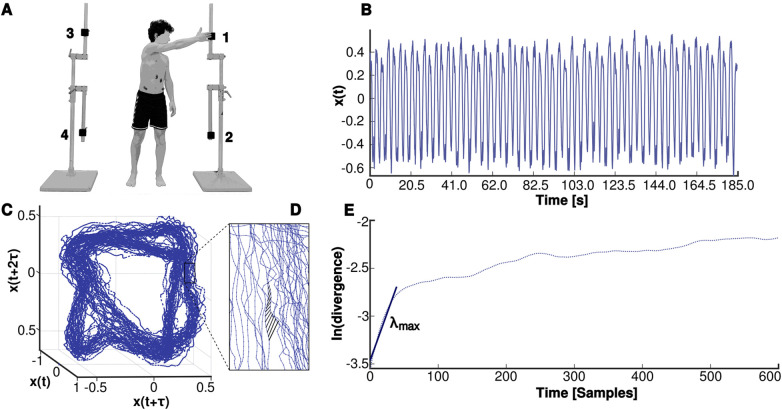
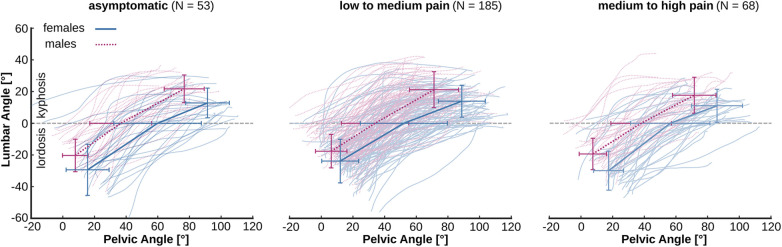
Methods: We measured lumbo-pelvic kinematics during trunk flexion and trunk dynamic stability and movement variability during a cyclic pointing task in 306 adults (156 females) aged between 18 and 64 years, reporting either no low-back pain or pain in the lumbar area of the trunk. Participants were grouped based on their characteristic pain intensity as asymptomatic (ASY, N = 53), low to medium pain (LMP, N = 185) or medium to high pain (MHP, N = 68). Participants with low-back pain that persisted for 12 weeks or longer were categorized as chronic (N = 104). Data were analyzed using linear mixed models in the style of a two way anova.
Results: Female participants showed a higher range of motion in both the trunk and pelvis during trunk flexion, as well as an increased lumbar lordosis in standing attributed to a higher pelvic angle that persisted throughout the entire trunk flexion movement, resulting in a longer duration of lumbar lordosis. The intensity and chronicity of the pain had a negligible effect on trunk posture and the lumbo-pelvic coordination. Pain chronicity had an effect on trunk dynamic stability (i.e., increased trunk instability), while no effects of sex and pain intensity were detected in trunk dynamic stability and movement variability.
Conclusions: Low-back pain intensity and chronicity was not associated with lumbo-pelvic posture and kinematics, indicating that lumbo-pelvic posture and kinematics during a trunk flexion movement have limited practicality in the clinical diagnosis and management of low-back pain. On the other hand, the increased local instability of the trunk during the cyclic coordination task studied indicates control errors in the regulation of trunk movement in participants with chronic low-back pain and could be considered a useful diagnostic tool in chronic low-back pain.
Keywords: lordosis; lumbo-pelvic rhythm; spine alignment; trunk stability; trunk variability.
© 2025 Fischer, Schroll, Schmidt and Arampatzis.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
How consistent are lordosis, range of movement and lumbo-pelvic rhythm in people with and without back pain?BMC Musculoskelet Disord. 2016 Sep 22;17(1):403. doi: 10.1186/s12891-016-1250-1. BMC Musculoskelet Disord. 2016. PMID: 27658946 Free PMC article.
-
Trunk muscle strength and lumbo-pelvic kinematics in adolescent athletes: Effects of age and sex.Scand J Med Sci Sports. 2019 Nov;29(11):1691-1698. doi: 10.1111/sms.13503. Epub 2019 Jun 27. Scand J Med Sci Sports. 2019. PMID: 31206810
-
Comparison of lumbo-pelvic kinematics during trunk forward bending and backward return between patients with acute low back pain and asymptomatic controls.Clin Biomech (Bristol). 2017 Jan;41:66-71. doi: 10.1016/j.clinbiomech.2016.12.005. Epub 2016 Dec 10. Clin Biomech (Bristol). 2017. PMID: 27992778 Free PMC article.
-
Lumbo-pelvic proprioception in sitting is impaired in subgroups of low back pain-But the clinical utility of the differences is unclear. A systematic review and meta-analysis.PLoS One. 2021 Apr 26;16(4):e0250673. doi: 10.1371/journal.pone.0250673. eCollection 2021. PLoS One. 2021. PMID: 33901255 Free PMC article.
-
Kinematic Characteristics of Sit-to-Stand Movements in Patients With Low Back Pain: A Systematic Review.J Manipulative Physiol Ther. 2019 Sep;42(7):532-540. doi: 10.1016/j.jmpt.2018.12.004. J Manipulative Physiol Ther. 2019. PMID: 31864436
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392(10159):1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease Study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396(10267):2006–17. 10.1016/S0140-6736(20)32340-0 - DOI - PMC - PubMed
-
- Aksekili MAE. Low back pain. In: Longo UG, Denaro V, editors. Textbook of Musculoskeletal Disorders. Cham: Springer International Publishing; (2023). p. 329–37. 10.1007/978-3-031-20987-1_37 - DOI
-
- Al Ameri K, Al Memari S. Performing back physical examination. In: Lari S, Al Memari S, Al Marzooqi D, editors. Family Medicine OSCE: First Aid to Objective Structured Clinical Examination. Singapore: Springer Nature; (2024). p. 299–300. 10.1007/978-981-99-5530-5_78 - DOI
LinkOut - more resources
Full Text Sources