

This is a preprint.
Prognostic Features in Surgically Resected Well-Differentiated Pancreatic Neuroendocrine Tumors: An Analysis of 904 Patients with 7882 Person-Years of Follow-Up
- PMID: 40236435
- PMCID: PMC11998843
- DOI: 10.1101/2025.04.01.25325055
Prognostic Features in Surgically Resected Well-Differentiated Pancreatic Neuroendocrine Tumors: An Analysis of 904 Patients with 7882 Person-Years of Follow-Up
Update in
-
Prognostic Features in Surgically Resected Well-Differentiated Pancreatic Neuroendocrine Tumors: an Analysis of 904 Patients with 7882 Person-Years of Follow-Up.Endocr Pathol. 2025 Jun 27;36(1):24. doi: 10.1007/s12022-025-09866-z. Endocr Pathol. 2025. PMID: 40576906 Free PMC article.
Abstract
Importance: The clinical behavior of well-differentiated pancreatic neuroendocrine tumors (PanNETs) is difficult to predict.
Objective: To define more accurately prognosticators for patients with a surgically resected PanNET.
Design: The pathology and Ki-67 immunolabeling index of PanNETs resected from 904 patients was correlated with patient outcome.
Setting: Academic tertiary care hospital.
Participants: Consecutive patients who had a PanNET resected between 1985 and 2025.
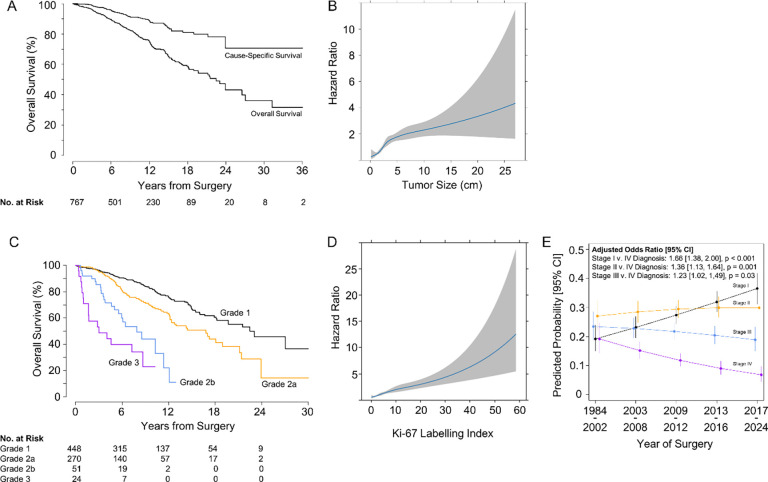
Results: The mean patient age at surgery was 56.6 years (SD 14.0), 477 were male (52.8%), and 7882 person-years of follow-up were obtained (mean 8.8 years, SD 6.5). The 10-year survival was 81% (95% CI: 77,86%) for patients with G1 PanNETs (Ki-67 <3%), 68% (95% CI: 61,76%) for patients with G2a PanNETs (Ki-67 3- <10%), 44% (95% CI: 29,66%) for patients with G2b PanNETs (Ki-67 of 10%- ≤20%), and 23% (95% CI: 8,61%) for patients with G3 PanNETs. Metastases (HR 4.7, p <0.0001), vascular invasion (HR 3.0, p <0.0001), tumor size ≥ 2 cm (HR 2.88, p <0.0001), perineural invasion (HR 2.42, p<0.0001), and positive margins (HR 2.18, p <0.0001) were associated with worse overall survival. Insulinoma (HR 0.34, p=3e-04), sclerosing variant (HR 0.47, p=0.05), and cystic variant (HR 0.61, p=0.05) were associated with improved overall survival. T stage and N stage were all statistically significant classifiers of overall survival. Similar associations were found with respect to disease relapse. There was a significant (P<0.001) increase in the proportion of patients diagnosed with stage I vs stage IV disease over time.
Conclusions and relevance: This study supports the classification of PanNETs into four grades (G1, G2a, G2b, and G3) based on Ki-67 labeling, which allows a more accurate prognostic assessments of patients.
Keywords: Ki 67; PanNET; Well-differentiated pancreatic neuroendocrine tumor; grade; prognosis; stage; vascular invasion.
Figures
References
-
- Pathak S, Starr JS, Halfdanarson T, Sonbol MB. Understanding the increasing incidence of neuroendocrine tumors. Expert Rev Endocrinol Metab. 2023;18(5):377–385. - PubMed
-
- Thiis-Evensen E, Boyar Cetinkaya R. Incidence and prevalence of neuroendocrine neoplasms in Norway 1993–2021. J Neuroendocrinol. 2023;35(4):e13264. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources