

Validation of High Ischemic and Bleeding Risk Criteria of European Guidelines in Peripheral Arterial Disease
- PMID: 40237688
- PMCID: PMC12287741
- DOI: 10.1016/j.jacasi.2025.01.018
Validation of High Ischemic and Bleeding Risk Criteria of European Guidelines in Peripheral Arterial Disease
Abstract
Background: The 2024 European Society of Cardiology (ESC) guidelines for peripheral arterial disease (PAD) propose the dedicated high ischemic risk (HIR) and high bleeding risk (HBR) criteria.
Objectives: The purpose of this study was to validate the ESC-HIR and HBR criteria using real-world data.
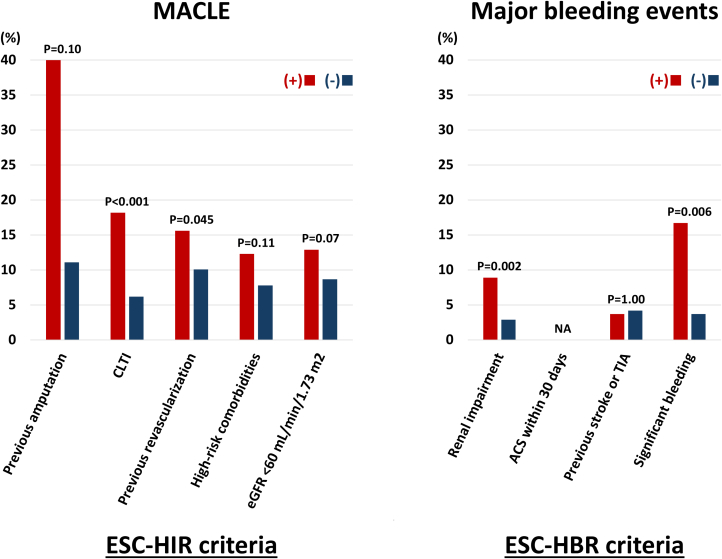
Methods: From January 2019 to December 2022, this multicenter retrospective registry included 824 patients undergoing endovascular treatment for aortoiliac and femoropopliteal PAD. The ESC-HIR criteria include previous amputation, critical limb-threatening ischemia, previous revascularization, high-risk comorbidities (heart failure, diabetes, polyvascular disease), and estimated glomerular filtration rate <60 mL/min/1.73 m2, while the ESC-HBR criteria include dialysis or renal impairment (estimated glomerular filtration rate <15 mL/min/1.73 m2), acute coronary syndrome <30 days, history of stroke or transient ischemic attack, and active or clinically significant bleeding. Although patients were initially divided into 4 groups according to the presence or absence of HIR and HBR, patients with HBR and no HIR were excluded caused by the small sample size (n = 2). Major adverse cardiovascular and limb events and bleedings were evaluated.
Results: Of the 822 patients, 62 (7.5%), 467 (56.8%), and 293 (35.6%) were grouped in the HIR (-)/HBR (-), HIR (+)/HBR (-), and HIR (+)/HBR (+). During the median follow-up period of 726 days, major adverse cardiovascular and limb events occurred in 0%, 9.5%, and 16.4% among the 3 groups (P = 0.005). The incidence of major bleeding events was 4.8%, 2.4%, and 6.8%, respectively (P = 0.009).
Conclusions: The ESC-HIR and HBR criteria successfully stratified ischemic and bleeding risks in patients with PAD undergoing endovascular treatment.
Keywords: guidelines; peripheral arterial disease; risk stratification.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures






Similar articles
-
Infusion techniques for peripheral arterial thrombolysis.Cochrane Database Syst Rev. 2021 Nov 17;11(11):CD000985. doi: 10.1002/14651858.CD000985.pub3. Cochrane Database Syst Rev. 2021. PMID: 34786692 Free PMC article.
-
Antiplatelet agents for preventing thrombosis after peripheral arterial bypass surgery.Cochrane Database Syst Rev. 2015 Feb 19;2015(2):CD000535. doi: 10.1002/14651858.CD000535.pub3. Cochrane Database Syst Rev. 2015. PMID: 25695213 Free PMC article.
-
Ticagrelor monotherapy versus ticagrelor plus aspirin in patients with chronic coronary syndrome and high ischaemic risk: a post hoc analysis of the TWILIGHT trial.EuroIntervention. 2025 May 16;21(10):550-559. doi: 10.4244/EIJ-D-24-00973. EuroIntervention. 2025. PMID: 40375766 Clinical Trial.
-
Antiplatelet and anticoagulant drugs for prevention of restenosis/reocclusion following peripheral endovascular treatment.Cochrane Database Syst Rev. 2012 Aug 15;2012(8):CD002071. doi: 10.1002/14651858.CD002071.pub3. Cochrane Database Syst Rev. 2012. PMID: 22895926 Free PMC article.
-
Glucagon-like peptide 1 (GLP-1) receptor agonists for people with chronic kidney disease and diabetes.Cochrane Database Syst Rev. 2025 Feb 18;2(2):CD015849. doi: 10.1002/14651858.CD015849.pub2. Cochrane Database Syst Rev. 2025. PMID: 39963952
Cited by
-
Regional Heterogeneity in the Risk of Thrombosis and Bleeding in Patients With Peripheral Artery Disease.JACC Asia. 2025 May 7;5(6):755-7. doi: 10.1016/j.jacasi.2025.03.007. Online ahead of print. JACC Asia. 2025. PMID: 40396938 Free PMC article.
References
LinkOut - more resources
Full Text Sources
